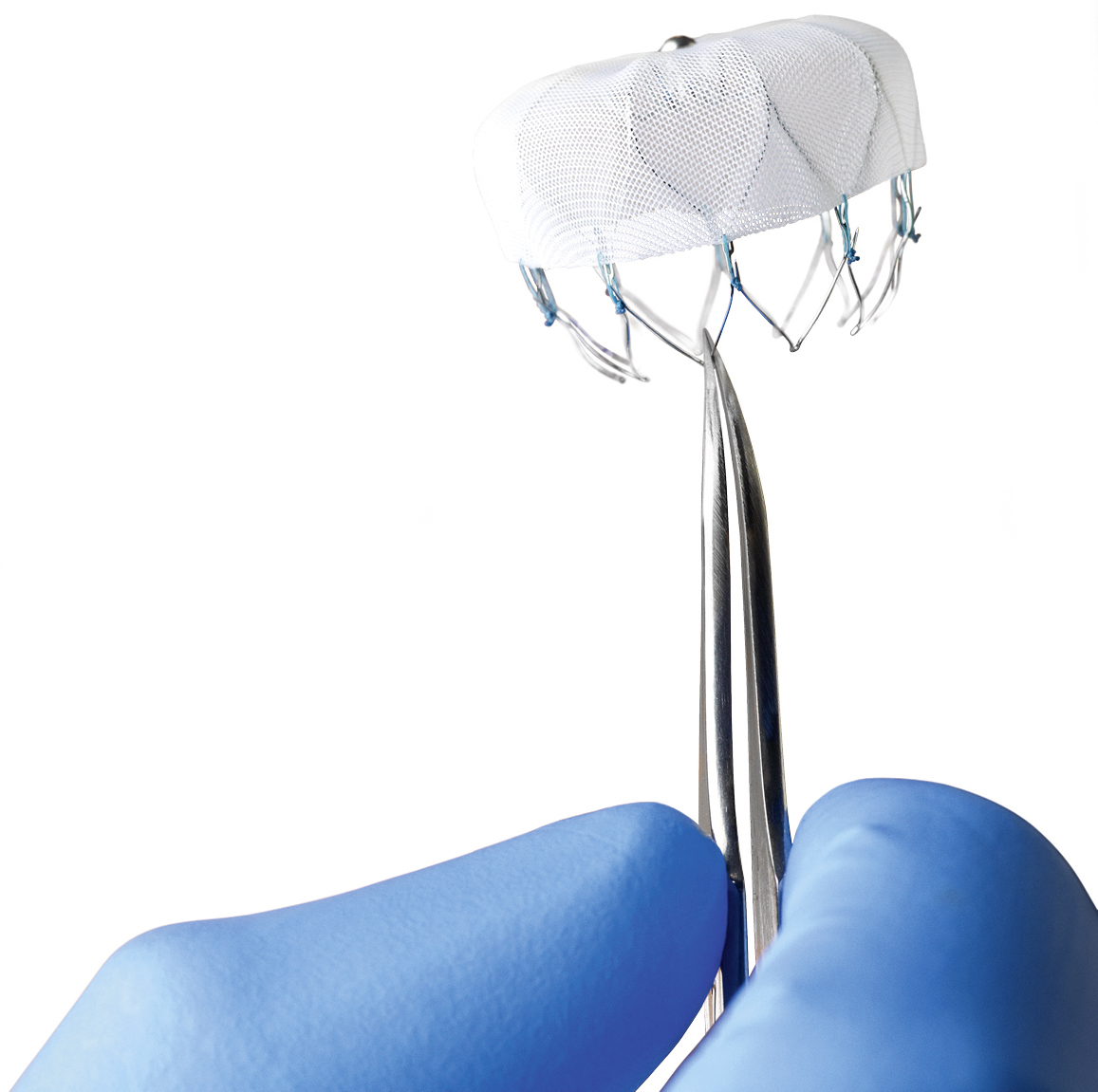
What is it? The Watchman, by Boston Scientific is a little device, sort of like a basket, that can be inserted into the left atrial appendage, theoretically blocking it off and preventing clot formation. As you probably know already, clot formation may lead to Stroke. The device was FDA approved in the US in March, 2015, and has been used in Europe since 2005.
It’s placed in the left atrial appendage via a catheter through an artery in the groin, and if all goes well the patient can discontinue their blood thinner (warfarin, etc.) within six months.
Sounds great, doesn’t it?
I know I’d love to be protected from having another TIA or stroke and not have to take a blood thinner – I’m currently on warfarin + aspirin which makes bicycling, especially mountain biking, quite hazardous. But truthfully, it’s not that I necessarily want to be off the warfarin: I just don’t want to ever have another TIA/stroke. Recall that I had my event while I was already taking Pradaxa (and I never missed a dose). I just want a treatment that is going to work.
But there is some evidence to suggest the Watchman might not be as terrific as it sounds.
A recent study showed that the risk of a major bleed over the course of three years is the same with the Watchman compared to just staying on warfarin. Huh?
Patients with atrial fibrillation (AF) who received a left atrial appendage closure device (Watchman, Boston Scientific) or stayed on long-term warfarin therapy had similar rates of major bleeding during a mean follow-up of 3.1 years, in pooled analysis of two randomized clinical trials[1]. However, patients who received the device and were able to stop taking warfarin and clopidogrel at 6 months had lower rates of major bleeding from then onward, compared with patients receiving long-term warfarin.
Furthermore, in a very thoughtful, somewhat technical, article CMS Proposal on Watchman Is the Right Decision, Dr John Mandrola, a thought leader in Cardiology and Electrophysiology, agrees with the CMS proposal that “the evidence is sufficient to determine percutaneous left atrial appendage closure therapy using an implanted device is not reasonable and necessary.”
There are two major studies in the US regarding the Watchman. According to Dr Mandrola in the PREVAIL study, “Due to an excess of ischemic strokes, Watchman did not reach noninferiority in this category in the updated analysis presented to the FDA.” In PROTECT-AF study, “ischemic strokes were numerically higher in the Watchman group.” Which, ultimately, “leads one to conclude that the device is not effective.”
As for me, personally, as much as I’d like to believe the Watchman is a solution for me, the evidence, so far, is not convincing. I’m going to wait.
By the way, if any readers have experience with the Watchman PLEASE leave a comment below. We would love to hear from you!
“The main adverse events related to this procedure are pericardial effusion, incomplete LAA closure, dislodgement of the device, blood clot formation on the device requiring prolonged oral anticoagulation, and the general risks of catheter-based techniques (such as air embolism). The left atrium anatomy can also preclude use of the device in some patients.”
By the way – I linked a couple of articles from Medscape. I’m not certain but I think you need to be registered for that sight. Sorry.
As a distance runner with atrial fibrillation, who never missed a single dose of my anti-coagulant, and who has already had a blood clot in my left atrial appendage, and has already had a “mini-stroke” – this one leaves me feeling a bit hopeless.
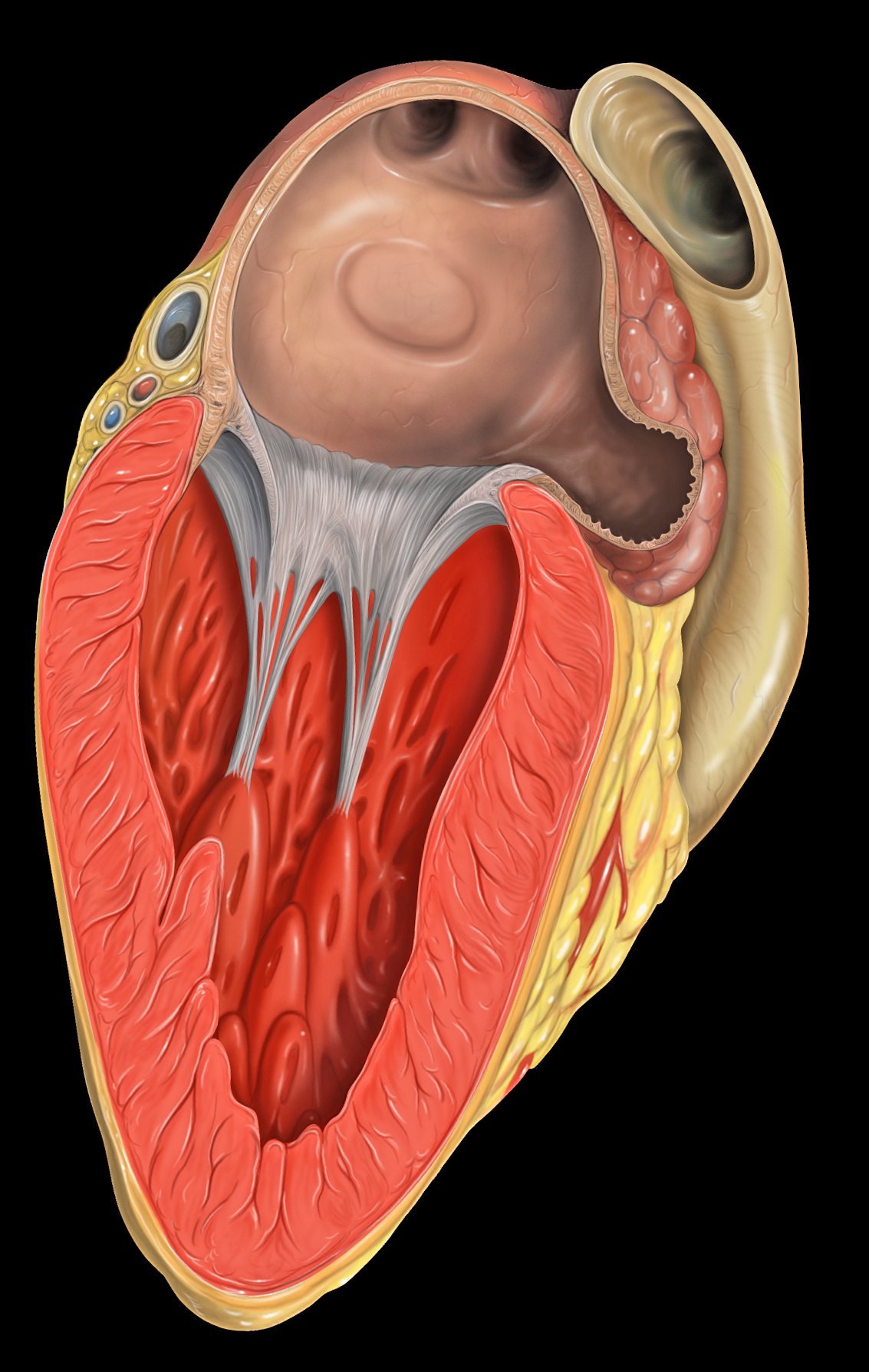
Feel free to read the article; but I will go over a few key points here. One of the dreaded consequences of atrial fibrillation is having a stroke. Because the top chambers of the heart, the atria (plural of atrium) are beating so fast that they are basically just sitting there vibrating, the blood pools and becomes sluggish, and is prone to forming blood clots. Combine this with an enlarged left atrium and the likelihood is even higher. The blood clot forms in a little corner of the heart called the “left atrial appendage” (LAA).
That’s where I formed a clot. If the blood clot, or a piece of the clot, breaks off it can quickly travel to the brain, get caught and cut off the circulation to part of the brain. This is a type of stroke, and is a huge problem for people with atrial fibrillation.
There are people who like to refer to a stroke as a “brain attack” because that’s what it is – like a heart attack in the brain. And like heart attacks there are big ones and small ones. I had a small one (TIA – tangent ischemia episode) that fortunately only lasted a minute or so. A big stroke, of course, can be fatal.
Important point: if a person is in atrial fibrillation and has blood clot in the LAA, it might be very stable. It might be just sitting there, hanging out, because the atria isn’t doing any beating. Everything is pretty tranquil in there. But then the person has a cardioversion (shock to reset the beating heart) or an ablation and the atrium begins to beat again, the blood starts moving through more quickly – well – now there’s a problem. Now the clot can break loose and BLAM!! – you’ve had a stroke!
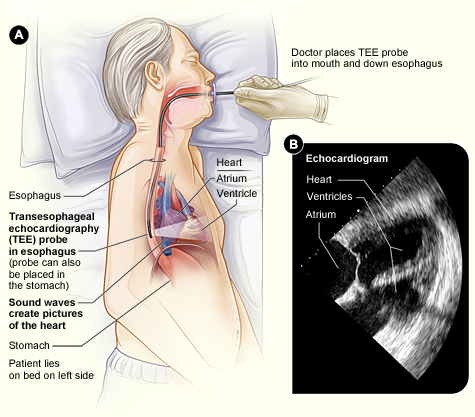
The problem: it’s difficult to tell whether or not a patient has a clot prior to having a procedure. A regular echocardiogram doesn’t even show a small clot; there’s not enough detail. The best way to determine if a clot is present is to do a transesophageal echocardiogram (TEE).
Transesophageal Echocardiogram
I’ve had three TEEs – it’s not fun – sort of like swallowing a telephone. Thankfully the last two that I had involved an anesthesiologist who put me to sleep for the procedure.
As far as I know it is fairly common to have a TEE prior to having an ablation procedure; but less common before a cardioversion (the shock!), especially for people who presumably have a low risk of a LAA blot clot – like people who are appropriately anti-coagulated, or people who have had atrial fibrillation for less that 48 hours.
In this article five interesting cases are reviewed.
Case #1 – a patient who was effectively anti-coagulated but turned out to have a LAA clot anyway (sounds familiar).
Case #2 – a patient who was actually more anti-coagulated than thought necessary, and was in atrial flutter for less than 48 hours, but turned out to have a LAA clot anyway.
Case #3 – an appropriately anti-coagulated person with a low risk of clot (CHADS2 score=1), but turned out to have a LAA clot anyway.
Cases #4 and #5 were high risk patients who would be expected to have a high risk of a clot. Case #5 actually had three clots in her heart – yikes!
How does all this apply to athletes with atrial fibrillation? Well, apparently healthy, athletic patients, who are appropriately anti-coagulated, and either undergoing a planned or emergency cardioversion, still have a certain risk of having a LAA clot and subsequent stroke.
Should everybody have a TEE before having a cardioversion? Probably not. TEE is expensive, unpleasant, and if anesthesia is involved it basically takes up an entire day out of your schedule. It might be a good idea to talk it over with your cardiologist, however.
A week or so ago I re-certified in ACLS – Advanced Cardiac Life Support. ACLS is a set of emergency clinical interventions for cardiac arrest, stroke, respiratory arrest, etc., which is basically a step above BLS (Basic Life Support – formerly known as CPR). ACLS certification, in my case anyway, is done through the American Heart Association, and is only open to health care providers: doctors, nurses, dentists, advanced practice providers like PAs and nurse practitioners, EMTs, respiratory therapists, pharmacists, and so on.
I thought I’d write about it in this blog so people might know what to expect as far as the type of treatment they might experience if they have an unstable episode of atrial fibrillation.
I’m in permanent atrial fibrillation, so when I’m in one of these classes I’m glad I’m not hooked up to an EKG – I don’t feel like getting medicated or shocked!
ACLS deals with various problems using algorithms, so let’s look at the “Tachycardia with a Pulse Algorithm” which would generally apply to acute atrial fibrillation.
So basically we start with a person with a fast heart rate. Tachycardia is, by definition, a pulse over 100 beats per minute, but for ACLS purposes it generally means a pulse over 150 bpm. Obviously not all tachycardia (fast heart rate) is atrial fibrillation.
For this article I am not discussing the other types of tachycardia, even though they are in the algorithm. I assume most people reading this blog are dealing with atrial fibrillation.
The first step is to assess the patient, identify and treat any underlying cause, make sure the patient is breathing effectively, assist if necessary, and give the patient some oxygen.
Now the next step is very important – is the patient stable? Five things: 1.) Is the blood pressure too low? 2.) Is there altered mental status (confusion)? 3.) Is the patient going into shock? 4.) Chest pain? 5.) Heart failure?
Even though I am in atrial fibrillation, all the time, I don’t have any of these symptoms. But if the patient is unstable and have tachycardia, basically, they are going to be getting some electricity! That means synchronized cardioversion, and in the case of atrial fibrillation (see “narrow irregular”) that means 120-200 joules – that’s a big shock!
Notice that it says “consider sedation.” Sedation can be considered, but not if it interferes with getting the unstable patient shocked as soon as possible. If you go into unstable atrial fibrillation at a race expect that the sedation will likely be skipped and get ready to be ZAPPED.
Photo by Ted Friedman.
This is for unstable tachycardia – that means the patient is in some sort of crisis that may eventually be life threatening.
For an episode of stable atrial fibrillation expect vagal maneuvers and a referral to a cardiologist. Vagal maneuvers include firm carotid sinus massage, coughing, gagging, valsalva maneuver (holding your breath and “bearing down”), and placing your face in ice water (snow also works). A lot of people with intermittent atrial fibrillation already know how to do this.
I’d be very interested in anybody else’s experience with unstable atrial fibrillation and what type of treatment was administered. Please comment below. Thanks.
I’m going to “ring my own bell” here and post that afibrunner.com has been chosen, once again, as one of Healthline’s The Best Atrial Fibrillation Blogs of the Year. Thanks so much, Healthline!
According to my WordPress dashboard I have a lot of views of my blog directed from healthline.com – I truly appreciate it.
It’s been a while since I have written and I have to say the last couple of months have been nerve-wracking. As I posted in a previous entry I had a TIA (transient ischemic attack) while running a couple of months ago, had a normal carotid scan, but a TEE (trans-esophageal echocardiogram) showed that I had a small blood clot in my left atrial appendage.
In other words I had a “mini-stroke” and was at risk of having a full on stroke.
This TIA occurred while I was on Pradaxa, a newer, novel anticoagulant. At that point I was taken off Pradaxa, started on Lovenox (low molecular weight heparin) injections, and warfarin (Coumadin), and also aspirin. I was instructed to discontinue running, and bicycling, and limit my activity to easy walks, and a repeat TEE was scheduled two months after the initial one.
I won’t hold back any longer regarding the surprise ending – I never had a second TIA “mini-stroke” (that I know of) or stroke and the follow-up TEE (trans-esophageal echocardiogram) showed that the blood clot inside my heart is now gone. Hooray!
Photo – The little cul-de-sac is the LA appendage
Just to review how this happens: when you are in atrial fibrillation your atria is beating so fast it’s like it isn’t beating at all, just sort of vibrating. There is a part of the left atrium (the “appendage”) where the blow flow is extra sluggish, and this is where clots can form. When a tiny piece of clot breaks of and goes into the brain that’s a TIA. If a big clot is present and breaks of into the brain that’s a stroke, which of course can be disabling and even fatal.
It goes without saying that I am disappointed that this occurred while I was on Pradaxa. I figured that as long as I was taking it I was safe, and I liked not having to watch my diet or have blood tests constantly. Taking Pradaxa is easy – “set it and forget it.” Now I’m on warfarin (Coumadin), a royal pain in the butt, and have to micromanage my diet constantly – this drug is not an easy choice for a vegetarian! Eating too many greens (think kale) is dangerous as is not eating enough greens. Imagine trying to eat about the same amount of kale or broccoli or spinach each day.
Photo – vegan pizza
My target INR is between 2.0 and 3.0, but seeing as I have had a TIA while on an anticoagulant I am trying to keep it nearer to 3.0 or even higher (3.0 – 3.5).
The two months between echocardiograms was an era of angst – anxiety and fear – for me, especially the first several weeks. Every symptom, no matter how minor, seemed like stroke. For example – lie in bed trying to get to sleep and your hand becomes numb – normal, right? Not when you know you have a blood clot in your heart – that seems like a stroke! Jump up from bed, start testing the muscle strength in each arm and leg, recite the alphabet, smile, frown, move eyebrows up and down checking for asymmetry. Do you think I’m exaggerating?
Every once in a while a person stammers or mispronounces a word. Normal? Maybe, but not when you are obsessed with a gigantic blood clot lodging in your brain.
As far as exercise was concerned at first I was limiting myself to short, easy walks more appropriate for a non-athlete. Eventually I became a bit bolder and started doing longer (but slow, especially up hills) hikes of an hour or two. It took me three weeks (!) to bridge to a therapeutic INR, so I was on warfarin and Lovenox for all that time. Once I was off the injections I started doing bike rides – but they were on non-technical trails and were slow, especially while going uphill.
My brain never got the memo that I was no longer a long distance runner/cyclist so I still ate like I was, and consequently I’ve gained some weight.
At this point, after finding out the clot is no longer present, I have started increasing the intensity of my bike rides, but mostly I’m still doing bike rides. I haven’t yet started running again – but I will.
I am mountain biking again, but not on any trails that would be considered challenging. Well, that’s not 100% true, I guess.
Photo – “Adventure Without Limits?”
As far as mountain biking is concerned I am phasing out technical trails (gradually). I made a deal with my self that if I didn’t have the blood clot on the second TEE I would get a new bike – and I did. I got a Specialized AWOL, which is a “gravel grinder.” That’s sort of a cross between cyclocross bike and a loaded touring road bike – basically a bike designed for gravel or dirt roads – we have an infinite supply of these around here so I have a lot of exploring ahead of me.
As far as that blood clot is concerned I’m very pleased it has gone away – but I am not fooling myself that it is gone forever. It could return at any time. It wasn’t there when I had my second TEE, but it could actually be there right now – how would I know? How long had it been there and how many times have I had a clot in that area? There’s no telling without doing a ridiculously expensive, somewhat invasive test over and over. I guess all I can do is stay vigilant, take my meds, watch the diet, and keep on trying to run, hike, and ride, even if it is at a reduced level.
I’m a 64 year-old road/trail runner, marathoner and weight lifter diagnosed with atrial fibrillation more than a decade ago. I’ve had three ablations and as many cardioversions, plus I’ve swallowed the usual assortment of prescription meds. Now my a-fib has become paroxysmal atrial flutter—about one episode every two weeks or so, usually lasting a few hours—and while my running days seem to be over, I still regularly make it to the gym and I’m discovering the joys of walking and hiking.
Through trial and error—plenty of each, actually—as well as a fair amount of research, I’ve come to a handful of conclusions that may be useful. While I believe them to be true, keep in mind that my observations are true for me; your experience may well be different. Finally, since I’m not a physician, nothing here is intended as medical advice.
And now: 5 things I’ve learned in 10 years of dealing with the always-entertaining world of cardiac arrhythmia.
A-Fib won’t kill you…even though a diagnosis of a-fib—and its symptoms—can be very scary, barring underlying cardiac disease, a-fib is not inherently life-threatening. And so if you have just been diagnosed, relax as best you can.
…but a stroke could. Pay rigorous attention to your anti-coagulation regimen. Even if your CHAD score is zero, at least take a low-dose aspirin every day. Personally, I find Coumadin to be a true pain, what with blood monitoring, dietary restrictions and the like. I much prefer the newer meds, especially Xarelto. It acts quickly, and as an added bonus you don’t have to be continuously concerned with your INR numbers.
Your EP isn’t interested in prevention. Typically, EP’s are all about fixing stuff rather than prevention. Which is weird, because unless you’re on the younger side of 40 and/or your a-fib has been freshly discovered, one ablation usually won’t do the trick. Of course, I’m grateful to my two EP’s, one rated among the best in California and the other acknowledged as one of the best in the world. It’s just that neither one has ever expressed any interest in the contours of my life, including what my exercise habits happen to be, what sorts of supplements I take, or what my days are like. Now, I’m not looking for a new best friend, but it’s clear that for them I’m a unique problem to be solved rather than a unique human being. I’m not angry about it; after all, these docs chose a field in which their major interaction with patients occurs when the patient is unconscious.
Still, I believe the implication is clear: you are pretty much on your own when it comes to figuring out how to modify your life style, exploring vitamin/mineral supplementation, and gathering the latest non-nutsy information.
(BTW, in terms of info, two websites I recommend are Dr. John Madrola and The A-Fib Report. Dr. John is a younger EP who always has a thought provoking take on new developments in a-f treatment and research and The A-Fib Report is a readable compendium of international a-f research, written in lay language. It requires a nominal membership fee that’s well worth it.)
Supplementation could work for you. I haven’t thrown out my beta blocker (Sotalol AF, not regular Sotalol) but along the way I have had excellent results in controlling the frequency and duration of my atrial flutter episodes by supplementing with 200 mg of magnesium citrate in a pill taken at lunch and ¼ teaspoon of potassium citrate dissolved in water taken in the morning and again at dinnertime (Please note: ingesting too much potassium involves some quite severe health risks, so be careful.)
Life is good. But first, the bad news: as near as I can tell, nobody knows what causes atrial flutter. The gang of suspects spans endurance sports (!) to mysterious biochemical mechanisms that somehow encourage the formation of tissue substrates that make the electrical system of the heart go haywire. Researchers—and your EP, too–are just guessing, leaning on statistical correlations rather than employing demonstrable causal connections. Maybe cutting out caffeine will help you; maybe it won’t. Maybe abstaining from demon rum will prove to be the answer; maybe not. Obviously, if you are over-drinking, over stressing (like many of us who are into enduro sports) under sleeping or happen to be engaged in other deleterious deeds, changing your behavior is simply a good idea, a-fib or no a-fib. Just don’t expect that any one thing will be the answer.
The good news is, you can have a great life even with a-fib and a-flutter. No, I don’t love my a-flutter episodes; they are annoying and sometimes, even after a decade, still frightening. I don’t run anymore, but a long walk or a moderate—I know, I know, not my favorite word, either—hike turns out to be a lot of fun. No, I can’t put the same hemodynamic load on my heart that I used to, but I can still work up a nice funky sweat underneath the weight machines at the gym.
Besides, working out is only a part of life. My friendships, relationship with my son, work, and my love life (I’m getting married again, and I’m stoked!) are just as satisfying as ever.
Maybe more so.
Those of us with a-fib or a-flutter aren’t sick, not truly. Nor do we need to afraid.
So—live!
(Thanks to Linda for the inspiration. Thanks to you for reading.)
About two weeks ago I was out for my typical Saturday two hour trail run on Moore Mountain with my dogs. It was a fine day and I felt great, and with about ten minutes left in the run I ran into three of my friends who were out mountain biking. My friend Linda, a Physician Assistant, was trying out her fancy new mountain bike and we stopped to talk for a while. She showed me her new bike and I introduced her to my new dog. I noticed, and commented, that I was having a little trouble getting my mouth working properly. I didn’t have any trouble finding words, or even saying the words, but my tongue just felt sort of thick – especially with consonants like “R” that seem to be made in the back of the mouth. I immediately did my self inventory for asymmetry and muscle weakness and found none. I attributed it to having had one of those little, annoying white sores in my mouth, accompanied by some swollen glands and thought nothing of it.
Linda Cyclecross racing
I finished my run, which involved a fairly technical descent, ate my post-run Clif Bar, and went home where I noticed nothing amiss. I forgot about it until Linda texted me the following day asking how I was doing and saying she was worried about me. I assured her – I was fine!
The next Monday, at work, I thought I’d ask my friend and co-worker, Dr Zakir Ali, if he thought the incident was any reason for concern. Dr Ali is a neurologist who works a couple of days a week at the orthopedic clinic, where I work as a podiatrist.
He wasn’t as dismissive as I was about the incident and said that that was very suspicious for a TIE (transient ischemic episode). A TIE is basically a small, brief stroke, in this case likely caused by a small blood clot that resolves fairly quickly. Dr Ali said I should, at the very least, get an echocardiogram to see if there is a clot in my left atrium, and possibly a carotid artery scan as well.
I have been in permanent atrial fibrillation and on Pradaxa, a potent anticoagulant (blood thinner) for two years and had never missed a dose. I thought he may have been over reacting – and I had had an echocardiogram just two months ago.
But Dr Ali had told me, “You will never regret checking.”
And I agreed.
Okay.
So I called the on call cardiologist, explained what had happened, and he told me a standard echocardiogram would be useless as it won’t show a clot, and recommended a trans-esophageal echocardiogram, and also a carotid scan (ultrasound).
I mentioned that I had had a trans-esophageal echocardiogram before (in 1994!) and it was like swallowing a telephone. He said he’d get anesthesia involved and we set up both procedures not expecting to find anything.
So the carotid scan came first and was normal, as expected.
Last Wednesday I went to the hospital and checked in to Day Surgery – which was a peculiar and strange experience for me. I’ve been working there, as a surgeon, for the past twenty-five years, but this was my first time being there as a patient. It’s a little disorienting, and oddly embarrassing, to be on “the other side of the door.”
Anyway – Dr Vince Herr, the anesthesiologist, gave me some propofol so I don’t remember a thing; but when I woke up I was told that I had a small clot in my left atrial appendage, and turbulence in my left atrium as well. This was a surprise for everybody involved. Judging from my lab work and the bruises on my arms the Pradaxa seemed to be working – but evidently not well enough! And that “small clot” looked pretty big to me – downright dangerous.
Trail Running on the PCT
At that point I was immediately started on Lovenox injections twice daily (for six weeks!), the Pradaxa was discontinued, and I am beginning to take warfarin (Coumadin); and of course I stay on the beta blocker (carvedilol). My cardiologist gave me the first Lovenox injection right in the post-op area.
Also it looks like no running or bicycling for six weeks – which of course is devastating to me, emotionally, but – shit! – blood clot / stroke / potential death – yes, I am definitely sticking with the program!
The injections are easy to do, they burn a bit but don’t really hurt, and every injection leaves a bruise. Believe it or not I enjoy and look forward to each injection because I’m hopeful that they will be helpful.
I’m disappointed that the Pradaxa failed – it is much easier to take that warfarin. Remember that I am a vegetarian and one of my passions is eating healthy food, especially kale. Also everyday, up until now, I eat a little square of nori (seaweed – like the wrapper on sushi) thinking that it would be a good source of iodine as I don’t eat any seafood or use table salt. Kale and nori are probably the two worst foods to eat if you’re taking warfarin!
Taking warfarin is going to be a real challenge – changes will be made, changes that actually seem sort of unhealthy. The one advantage is that warfarin is, unlike Pradaxa, reversible, which is a true benefit in the case of a bike or auto crash, a GI bleed, a head injury, and so on.
Moore Park Trails
In six weeks the trans-esophageal echocardiogram will be repeated and hopefully the clot will be gone. If not some sort of procedure (by the electrophysiologist) is in store for me. Hopefully I will 1.) not die and 2.) get back to trail running. Until then my nerves are wracked worrying about having a major stroke!
I need to say that I feel incredibly blessed – if I hadn’t met my friends and stopped to chat I never would have known I was having a TIE. And if Linda hadn’t have texted me the next day I wouldn’t have ever pursued it, because I had, in my mind, completely dismissed it. And also – how many people actually have a neurologist right in their office who is willing to talk at any time?
Clearly I’m not through this yet – but in a way I feel I have already dodged a bullet. Really, if it weren’t for Linda that blood clot would have just kept getting bigger and who knows what would happen next? I might be dead by now. Even as it is now – who knows? But at least now I know I have a problem and the treatment plan has been changed.
So thanks, Linda!
Me and Linda in Costa Rica
I would appreciate any comments, especially shared experiences, you might have.
I am honored to have had an article published in the December 2014 issue of EP Lab Digest, a monthly journal for electrophysiologists and allied health professionals who work in electrophysiology labs.
The managing editor, Jodie Elrod, had approached me about writing a “patient perspective” article as she was familiar with my afibrunner blog. The article is basically a synthesis of material already presented in this blog, particularly my article called Atrial Fibrillation – A Visit to the Electrophysiologist.
I am delighted to have this opportunity to communicate with the EP community and promote my plea for empathy with respect to the endurance athletes afflicted with atrial fibrillation.
Thanks EP Lab Digest!
Also interesting – my cousin Chuckie, (an electrophysiologist – I’m sure they don’t call him “Chuckie” at work), who I mention in my article, had an article published in the November 2014 issue of EP Lab Digest.
I have been in permanent atrial fibrillation for a couple of years now, but only been taking an anticoagulant (Pradaxa). But things have changed and for the past month I have been on a beta blocker, carvedilol.
Prior to starting the carvedilol, while in permanent atrial fibrillation, I had been able to run two marathons and one ultramarathon (50K) without any more trouble than the normal marathon type suffering, but over the past six months I have noticed things have been changing. I’ve slowed down, even for me, and distances are getting harder. My last half marathon was a joke and I was at the end of the pack within the first two miles. After a run or mountain bike ride of an hour or more I would have problems afterwards – my blood pressure would drop and my pulse would stay high. After a long run, especially if it was a hot day (which they all are, recently) I would get so light-headed after standing up I sometimes had to grip onto something to remain standing.
A visit to the cardiologist, and a subsequent echocardiogram, revealed that my heart rate was increasing and my ejection fraction was decreasing, and for that reason the cardiologist wanted me to start on a beta blocker.
A beta blocker, in this case carvedilol, is a drug that reduces stress on the heart by slowing the heart rate, decreasing the force with which the heart beats, and reduces the tone of the arteries throughout the body. The end result is that blood pressure is reduced, as is heart rate. The heart needn’t work so hard.
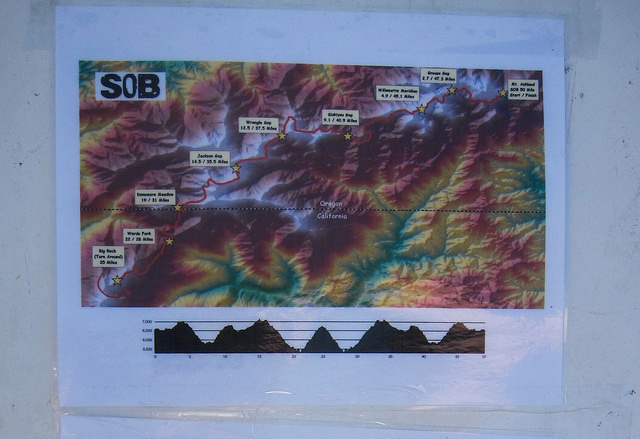
SOB 50 Mile Course – tough!
Some non-endurance athletes actually use beta blockers as performance enhancing drugs – it is said that it calms a person, reduces performance anxiety, and is commonly used in less endurance specific sports such as golf, target shooting, archery, and even in music performance.
Clearly these drugs are performance diminishing for endurance sports like distance running and mountain biking. We like to stress the heart, raise the heart rate, and we don’t have very much stress – we’re long distance runners after all – the mellowest people around.
I generally am in at least half marathon shape year round. Even if I’m not training for anything my weekend long run is going to be between nine and twelve trail miles. Prior to starting the beta blocker I had signed up for the 15K at the SOB Trail Run at Mount Ashland (Oregon) – one of my favorite races. This relatively high altitude run is basically all up and down trails and fire roads (zero flat sections) and I have done it at least six times in the past, including completing it twice in atrial fibrillation. I was curious to see how being on the beta blocker would affect my race.
DNF
The answer was I DNFed (did not finish) and dropped out fairly early in the race. That was terrible – most of my friends were running the 50K or the 50 mile and I DNFed the little 15K???
The course at the SOB is brilliant, really. A lot of trail races start out right away on singletrack, but the SOB has about a mile(?) of fire road at the start so everybody has plenty of time to figure out whether they are going to be running with the fast people or the slow people before they hit narrow Pacific Crest Trail. I ended up at the very back of the group that was running, but I was still in front of the few people who were walking the 15K.
I found that as soon as the course headed up hill I was unable to run. My chest felt funny – not chest pain, just felt weak, not right, and my legs felt dead. I wasn’t short of breath, I was just unable to do it. I decided, in my typical OCD mode, to continue running for five more songs on my iPod shuffle, and then turn around and drop out, thinking that I should at least get a little bit of a work out in, and that I could justify keeping the T-shirt I had paid extra for. I knew I could have walked the course, but that is not what I went there to do.
I was delighted that the fifth song on my iPod turned out to be an oldie from my high school days: Yours is No Disgrace by Yes. Not actually I song I still like very much, but in this context it seemed like a cosmic pat on the back.
On the way back I met a woman who was also DNFing (sprained ankle) and we walked the last section of the race together, commiserated, and removed our numbers so they wouldn’t mistake us for the top finishers. At the finish line we informed the race officials that we had dropped out so they didn’t need to send a search and rescue team to find us.
DNFing and commiserating together as we remove our race numbers
So this article is, basically, my first impression of being on a beta blocker, in addition to the atrial fibrillation, and trying to remain an endurance athlete.
So far I feel that the beta blocker is more of a hindrance to my running and cycling than the atrial fibrillation alone had been – but then again, because of the atrial fibrillation my heart function is gradually diminishing.
I should say, on a positive note, that the beta blocker is working, and is doing what it is supposed to do. I check my heart rate and blood pressure at least once per day and since I started the carvedilol I am right where the cardiologist wants me to be. And I can understand why people who aren’t trying to be athletes might like the med – it seems to have a mild calming effect. Furthermore I no longer feel like my heart is a fish flopping around in my chest, and my post work out blood pressure and heart rate has stabilized.
I am optimistic that the carvedilol will be worthwhile and will help me preserve and regain my ejection fraction. But really, what choice do I have?
So here is how things have changed so far (compared to just permanent a fib without the beta blocker):
1.) As far as mountain and road biking is concerned I have been able to ride all the hills that I used to be able to ride, although I am much slower. My wife now has to wait for me at the top of a climb, and that’s fine. I am delighted I can still ride and don’t have to get off and walk my bike.
2.) Running is more negatively influenced. My previous slow pace is even worse, and hills are quite difficult. Not surprisingly I do not like this one bit. A slow jog feels like a 5K effort. But I am still able to run – Yay!
3.) Long runs in heat are not possible. I am just not able to do a long run in heat, and lately every day has been warm. Understand that I am a big red-faced Irish-American who considers anything over sixty degrees to be hot running weather; plus I live in a very sunny place, a high desert climate without a lot of shade. It is not surprising that this is happening. A normal person running in heat will have a higher heart rate for a given pace, and will need to slow down. If you are on a beta blocker that reduces the maximum heart rate by a significant amount, well: “game over.”
My goal is to continue running and mountain biking on trails like this: Brown Mountain Trail
4.) I suspect that the beta blocker might be making me lazy. I don’t know if that is the right word, but I had a full day off in the middle of the week a while ago and I had planned on, among other things, writing this article and going for a trail run, and next thing I knew it was late afternoon and I hadn’t done a thing. What? By that time there was a thunderstorm so I was not going out for a run – but the article still hadn’t been started. I hope this is not going to be the case from now on. Being lazy and depressed is far from my idea of fun.
I am going to wait until I have had more experience with the beta blocker and write a better informed article. I’m going to sign up for a relatively flat (downhill, actually) trail half marathon and try to redeem myself.
In the meantime I would love hear about other people’s experiences with the dreaded beta blockers. Please post a comment below.
Is distance running therapeutic? Is mountain biking addictive? Is there such thing as a good addiction? If my atrial fibrillation worsens and I could no longer do long runs or bike rides – how hard would it be to kick the habit?
High Lakes Trail – Southern Oregon
Today in the hospital lounge, while I was eating some potato chips, somebody was telling me how bad potato chips are for me. Whatever – I have given up almost everything in the world that is bad for me. I haven’t drank alcohol in several years, haven’t smoked a cigarette in decades, gave up meat and eggs a couple of years ago, I’m almost dairy free, and I haven’t taken recreational drugs since high school in the seventies. Potato chips, which I feel are good enough to be “worth it,” are about it for me. Well, that and diet soda, which is also an unhealthy habit that I have.
But what about “runner’s high?” Is that my addiction?
And what exactly is runner’s high? Does it even exist? I’ve been hearing about it for a long time, even before I started running in the early 80s.
Allegedly the athlete’s brain is “flooded with endorphins, more powerful than any street drugs!”
Many distance runners claim to experience euphoria during or after running, and some claim they’ve never had it happen – not even once.
The endorphin theory is the oldest, but more recently I’ve read about how endocannabinoids (naturally occurring neurochemicals related, in a way, to the active ingredient in cannabis) might be the cause of runner’s high.
Whatever the cause, it certainly appears to be real.
Pacific Crest Trail via Brown Mountain Trail – Klamath County, Oregon
Ultrarunner Dean Karnazes describes the role that running has in his life: “Some seek the comfort of their therapist’s office, other head to the corner pub and dive into a pint, but I chose running as my therapy”
“I’m convinced that a lot of people run ultramarathons for the same reason they take mood-altering drugs. I don’t mean to minimize the gifts of friendship, achievement, and closeness to nature that I’ve received in my running carer. But the longer and farther I ran, the more I realized that what I was often chasing was a state of mind – a place where worries that seemed monumental melted away, where the beauty and timelessness of the universe, of the present moment, came into sharp focus.”
― Scott Jurek, Eat and Run: My Unlikely Journey to Ultramarathon Greatness
Actually, a recent New York Times article states that on good experimental evidence it has been finally determined that exercise does indeed produce a flood of endorphins in the brain. Lucky us!
Researchers in Germany, using advances in neuroscience, report in the current issue of the journal Cerebral Cortex that the folk belief is true: Running does elicit a flood of endorphins in the brain. The endorphins are associated with mood changes, and the more endorphins a runner’s body pumps out, the greater the effect.
I won’t review the article here, but please read it – an elegant experiment, and solid conclusions.
But irrespective of the cause, what is runner’s high and what does it mean to endurance athletes? Can a person become addicted to it?
Personally I feel that the term runner’s “high” is a misnomer. I would describe it better as an altered state of consciousness rather than a high. Maybe I’m splitting hairs but I have never felt intoxicated by endurance sports.
Euphoria might even be too strong of a term – but maybe not. There are times during and after running when everything appears exceptionally crisp and beautiful. That’s why I love trail running, in Oregon, in the wilderness – does that happen to people in health clubs running on treadmills?
After an hour or so even carb gels seem remarkably delicious!
Also – music becomes intensely enjoyable. I do run with an iPod and sometimes I feel I am going back to the days back in high school when I smoked pot and would listen, chemically enhanced, to suddenly amazing music on headphones. Except now instead of sitting in a darkened basement I’m moving through the woods. It’s funny – a lot of the music that, for me, is most enjoyable on long runs, is the same type of music that I believe would be most enjoyable to a person who is stoned. Sometimes a song sounds so good I’ll repeat play a song two or three times.
But another reason I don’t like the title “runner’s high” is it isn’t all euphoria, beauty, and music joy. I think the exercise induced altered state of consciousness can involve a certain amount of emotional lability. Here’s an example: once I was on a twenty mile trail run, and at mile sixteen an old song I hadn’t heard in years, Careful With That Axe, Eugene, started playing in my random shuffle. This very early, nine minute long Pink Floyd song is sort of a novelty song; a one chord song that slowly builds on a rising and falling bass line with a mellow organ playing over it. At one point a whispering voice says, “Careful with that axe, Eu-zhene.” And then there is this horrific screaming and dissonant guitar, and finally it evolves back to the mellow bass and organ. Back when I was in high school, if we had somebody over who had never heard the song before, we’d put it on and turn down the lights, and of course when the screaming began it would scare the crap out of the first time listener, and we’d all have a good laugh.
Well I knew all about what was going to happen during that song and wondered if I would start laughing when the “axe” section came up. Imagine my surprise when I burst into blubbering tears when the screaming began. I should state that this was shortly after my ex-wife (with whom I was still friendly) and her family had died in a horrible house fire – but honestly I wasn’t even thinking about that until the screaming in the song. I know I wouldn’t have been anywhere near that emotional if I hadn’t just put in sixteen hilly trail miles.
Other times while running something will strike me as funny I will begin laughing giddily – out there all by myself, or in the back of the pack at a marathon. Or an angry song will play and I’ll feel, like, GRRRRRRR!, become angry – quite a catharsis.
GRRRRRRRR!
So is exercise induced altered state of consciousness addictive? I’m thinking: yes.
C – Have you ever felt you needed to cut down on your running? A – Has anybody ever annoyed you or criticized your running? G – Have you ever felt guilty about your running? E – Have you ever felt you needed a run first thing in the morning (Eye-opener) to steady your nerves?
Well – I can honestly say I’ve never felt guilty about my running, but the rest of those questions, well . . . .
And I can state for the record that with my atrial fibrillation, and the likely progression of my a fib, including my upcoming need to be on a beta-blocker, I have been dreading the day when I am no longer able to run. Very depressing.
Biking in A Fib – like riding through mud
Aside from that I have a theory. I think it is obvious that not everybody will experience anything like a runner’s high. Clearly many people hate the way running makes them feel, and they are the people who think distance runners are completely nuts. And why wouldn’t they? Based on the time they ran two miles and felt nothing but fatigue and pain, and interpolating that up to, say, thirty-one miles, their obvious conclusion would be “WTF?” to use the parlance of our times.
Lyon’s Trail – Lava Beds National Monument
But as for myself, and I’m guessing most of the people who would be interested in this blog, the so-called runners high can be generally considered to be a gift.
Diversion: How to talk to your children about distance running: