
Note: This is a post I made on a couple of atrial fibrillation Facebook groups – specifically:
Healthy Hearties
and I’m including it here in the hopes that readers will be inspired to write and share. Thanks!

Joey and I hiking on the nearby Pacific Crest Trail
I write and maintain A Fib Runner (afibrunner.com) – a blog about atrial fibrillation and trail running, ultra running, mountain biking, and other endurance sports. Studies have shown that atrial fibrillation is much more common in middle-aged athletes than in non-athletic individuals of the same age – doesn’t seem fair, does it? I’m a marathoner, ultra-marathoner, hiker, mountain biker with permanent atrial fibrillation – and I blog about it.
I would like to request guest bloggers to submit articles. I’ve written a lot about *my* experience; but your experience is going to be unique and will be of great interest to readers of the blog. At this point I have had several people send me articles and they have been very popular – some of the most popular articles on my blog.
So here’s how it works: if you’d like to submit and article let me know via comment or message. I’ll send you my email and we can get started. If writing intimidates you that’s fine – just right it in your own voice, like you are writing a letter to a friend.
If you want to use your full name – great! A lot of athletes with atrial fibrillation come from a generation that values privacy a little more than millennials – that’s fine. My 58 year old life is an open book, but maybe yours isn’t – a first name or even a pseudonym is fine. I’ll edit the article for spelling, grammar, punctuation, etc., and send you a revised copy (if there any revisions) for your approval.
If you’d like to send photos I’ll let you know how I do that. Blogs need photos – but if you have none to share I will provide appropriate photos.
The article should be about your experience and NOT about giving medical advice. Personally, I try very hard to write as an A Fib Runner and not as a health care provider. If you are a cardiologist, or other type of health care provider, and would really like to make suggestions we can discuss that. Clearly there are some real liability issues with giving medical advice over the internet.
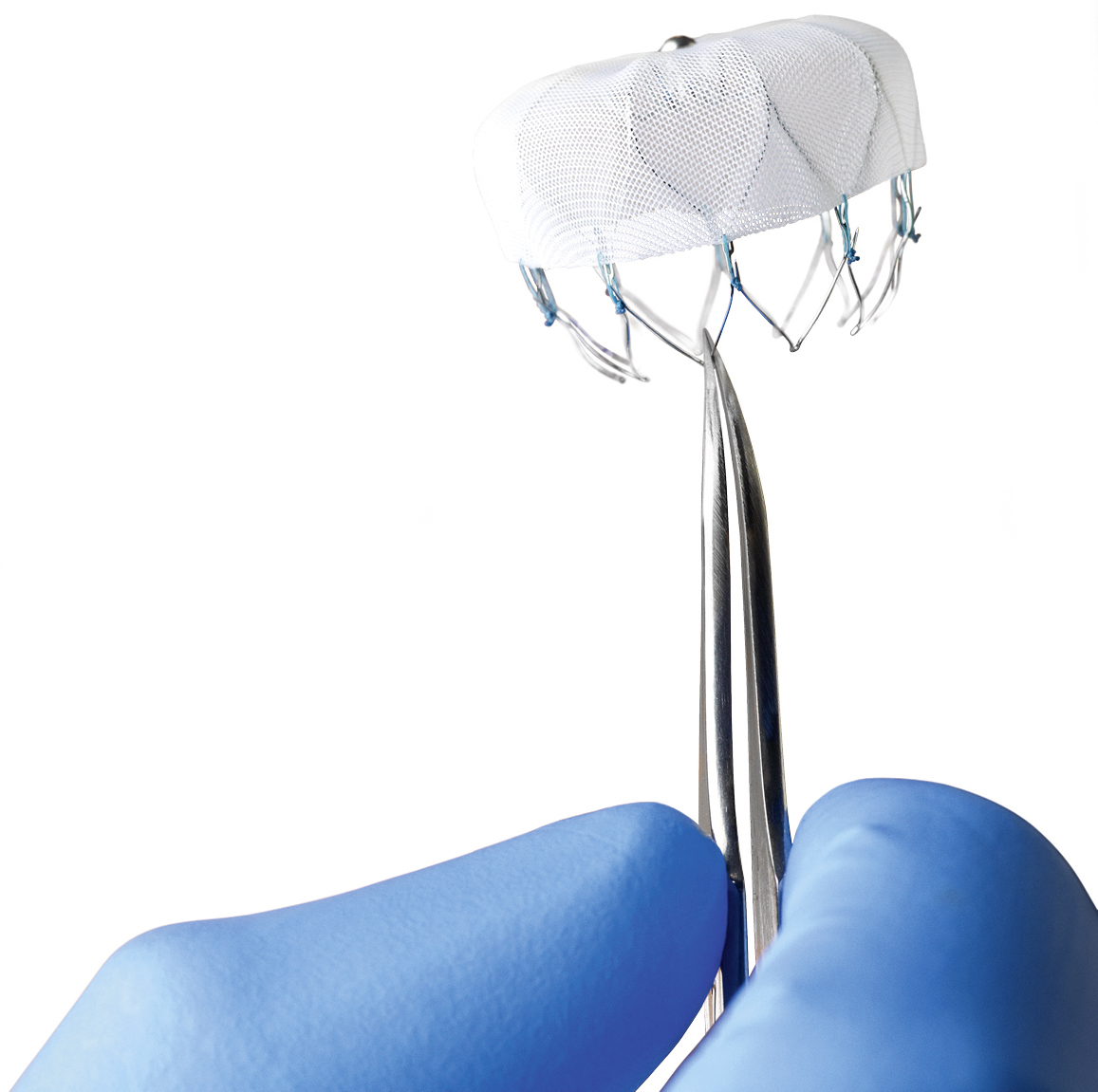
Any topic involving atrial fibrillation is appreciated, and I especially would like to hear from people who have had various treatments like ablation, a watchman device, or an Atriclip, as well as the various medications that you’ve used for atrial fibrillation. How did you find out you had a fib? What did it feel like? What is your emotional reaction to a fib? What is your psychological response to the new normal of a fib? What was your cardio version like? What are your triggers? What things did you change after the diagnosis was made? Did a fib destroy you or did it strengthen you?
And so on.
Please let me know – THANKS!



















{kind=link}