This is, so far, the most discouraging article about atrial fibrillation I have ever read:
As a distance runner with atrial fibrillation, who never missed a single dose of my anti-coagulant, and who has already had a blood clot in my left atrial appendage, and has already had a “mini-stroke” – this one leaves me feeling a bit hopeless.
Feel free to read the article; but I will go over a few key points here. One of the dreaded consequences of atrial fibrillation is having a stroke. Because the top chambers of the heart, the atria (plural of atrium) are beating so fast that they are basically just sitting there vibrating, the blood pools and becomes sluggish, and is prone to forming blood clots. Combine this with an enlarged left atrium and the likelihood is even higher. The blood clot forms in a little corner of the heart called the “left atrial appendage” (LAA).
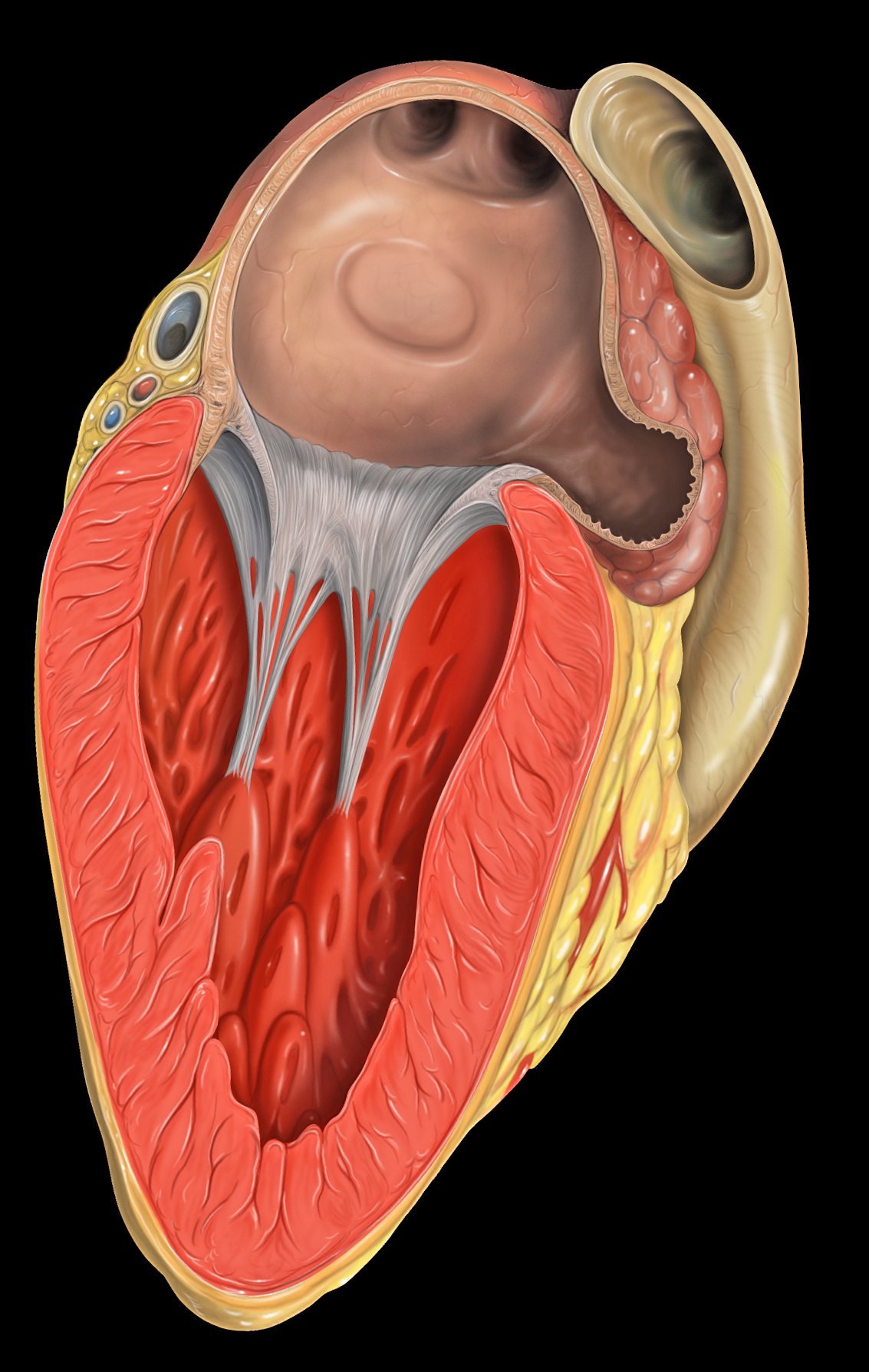
That’s where I formed a clot. If the blood clot, or a piece of the clot, breaks off it can quickly travel to the brain, get caught and cut off the circulation to part of the brain. This is a type of stroke, and is a huge problem for people with atrial fibrillation.
There are people who like to refer to a stroke as a “brain attack” because that’s what it is – like a heart attack in the brain. And like heart attacks there are big ones and small ones. I had a small one (TIA – tangent ischemia episode) that fortunately only lasted a minute or so. A big stroke, of course, can be fatal.
Important point: if a person is in atrial fibrillation and has blood clot in the LAA, it might be very stable. It might be just sitting there, hanging out, because the atria isn’t doing any beating. Everything is pretty tranquil in there. But then the person has a cardioversion (shock to reset the beating heart) or an ablation and the atrium begins to beat again, the blood starts moving through more quickly – well – now there’s a problem. Now the clot can break loose and BLAM!! – you’ve had a stroke!
The problem: it’s difficult to tell whether or not a patient has a clot prior to having a procedure. A regular echocardiogram doesn’t even show a small clot; there’s not enough detail. The best way to determine if a clot is present is to do a transesophageal echocardiogram (TEE).
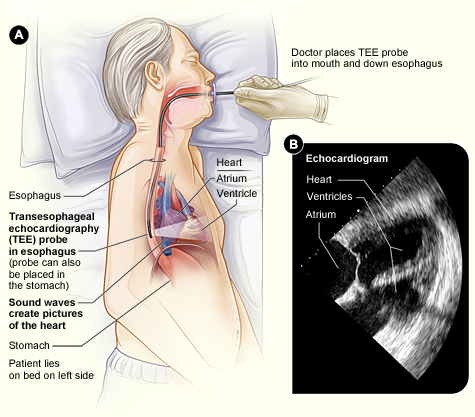 Transesophageal Echocardiogram
Transesophageal Echocardiogram
I’ve had three TEEs – it’s not fun – sort of like swallowing a telephone. Thankfully the last two that I had involved an anesthesiologist who put me to sleep for the procedure.
As far as I know it is fairly common to have a TEE prior to having an ablation procedure; but less common before a cardioversion (the shock!), especially for people who presumably have a low risk of a LAA blot clot – like people who are appropriately anti-coagulated, or people who have had atrial fibrillation for less that 48 hours.
In this article five interesting cases are reviewed.
Case #1 – a patient who was effectively anti-coagulated but turned out to have a LAA clot anyway (sounds familiar).
Case #2 – a patient who was actually more anti-coagulated than thought necessary, and was in atrial flutter for less than 48 hours, but turned out to have a LAA clot anyway.
Case #3 – an appropriately anti-coagulated person with a low risk of clot (CHADS2 score=1), but turned out to have a LAA clot anyway.
Cases #4 and #5 were high risk patients who would be expected to have a high risk of a clot. Case #5 actually had three clots in her heart – yikes!
How does all this apply to athletes with atrial fibrillation? Well, apparently healthy, athletic patients, who are appropriately anti-coagulated, and either undergoing a planned or emergency cardioversion, still have a certain risk of having a LAA clot and subsequent stroke.
Should everybody have a TEE before having a cardioversion? Probably not. TEE is expensive, unpleasant, and if anesthesia is involved it basically takes up an entire day out of your schedule. It might be a good idea to talk it over with your cardiologist, however.

Happy Trails