I am honored to have had an article published in the December 2014 issue of EP Lab Digest, a monthly journal for electrophysiologists and allied health professionals who work in electrophysiology labs.
The managing editor, Jodie Elrod, had approached me about writing a “patient perspective” article as she was familiar with my afibrunner blog. The article is basically a synthesis of material already presented in this blog, particularly my article called Atrial Fibrillation – A Visit to the Electrophysiologist.
I am delighted to have this opportunity to communicate with the EP community and promote my plea for empathy with respect to the endurance athletes afflicted with atrial fibrillation.
Thanks EP Lab Digest!
Also interesting – my cousin Chuckie, (an electrophysiologist – I’m sure they don’t call him “Chuckie” at work), who I mention in my article, had an article published in the November 2014 issue of EP Lab Digest.
I have been in permanent atrial fibrillation for a couple of years now, but only been taking an anticoagulant (Pradaxa). But things have changed and for the past month I have been on a beta blocker, carvedilol.
Prior to starting the carvedilol, while in permanent atrial fibrillation, I had been able to run two marathons and one ultramarathon (50K) without any more trouble than the normal marathon type suffering, but over the past six months I have noticed things have been changing. I’ve slowed down, even for me, and distances are getting harder. My last half marathon was a joke and I was at the end of the pack within the first two miles. After a run or mountain bike ride of an hour or more I would have problems afterwards – my blood pressure would drop and my pulse would stay high. After a long run, especially if it was a hot day (which they all are, recently) I would get so light-headed after standing up I sometimes had to grip onto something to remain standing.
A visit to the cardiologist, and a subsequent echocardiogram, revealed that my heart rate was increasing and my ejection fraction was decreasing, and for that reason the cardiologist wanted me to start on a beta blocker.
A beta blocker, in this case carvedilol, is a drug that reduces stress on the heart by slowing the heart rate, decreasing the force with which the heart beats, and reduces the tone of the arteries throughout the body. The end result is that blood pressure is reduced, as is heart rate. The heart needn’t work so hard.
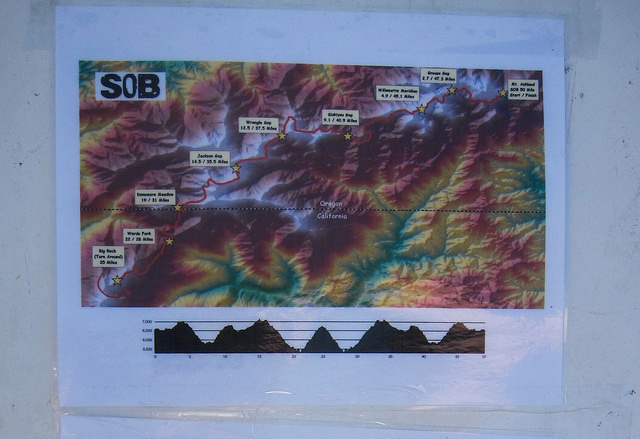
SOB 50 Mile Course – tough!
Some non-endurance athletes actually use beta blockers as performance enhancing drugs – it is said that it calms a person, reduces performance anxiety, and is commonly used in less endurance specific sports such as golf, target shooting, archery, and even in music performance.
Clearly these drugs are performance diminishing for endurance sports like distance running and mountain biking. We like to stress the heart, raise the heart rate, and we don’t have very much stress – we’re long distance runners after all – the mellowest people around.
I generally am in at least half marathon shape year round. Even if I’m not training for anything my weekend long run is going to be between nine and twelve trail miles. Prior to starting the beta blocker I had signed up for the 15K at the SOB Trail Run at Mount Ashland (Oregon) – one of my favorite races. This relatively high altitude run is basically all up and down trails and fire roads (zero flat sections) and I have done it at least six times in the past, including completing it twice in atrial fibrillation. I was curious to see how being on the beta blocker would affect my race.
DNF
The answer was I DNFed (did not finish) and dropped out fairly early in the race. That was terrible – most of my friends were running the 50K or the 50 mile and I DNFed the little 15K???
The course at the SOB is brilliant, really. A lot of trail races start out right away on singletrack, but the SOB has about a mile(?) of fire road at the start so everybody has plenty of time to figure out whether they are going to be running with the fast people or the slow people before they hit narrow Pacific Crest Trail. I ended up at the very back of the group that was running, but I was still in front of the few people who were walking the 15K.
I found that as soon as the course headed up hill I was unable to run. My chest felt funny – not chest pain, just felt weak, not right, and my legs felt dead. I wasn’t short of breath, I was just unable to do it. I decided, in my typical OCD mode, to continue running for five more songs on my iPod shuffle, and then turn around and drop out, thinking that I should at least get a little bit of a work out in, and that I could justify keeping the T-shirt I had paid extra for. I knew I could have walked the course, but that is not what I went there to do.
I was delighted that the fifth song on my iPod turned out to be an oldie from my high school days: Yours is No Disgrace by Yes. Not actually I song I still like very much, but in this context it seemed like a cosmic pat on the back.
On the way back I met a woman who was also DNFing (sprained ankle) and we walked the last section of the race together, commiserated, and removed our numbers so they wouldn’t mistake us for the top finishers. At the finish line we informed the race officials that we had dropped out so they didn’t need to send a search and rescue team to find us.
DNFing and commiserating together as we remove our race numbers
So this article is, basically, my first impression of being on a beta blocker, in addition to the atrial fibrillation, and trying to remain an endurance athlete.
So far I feel that the beta blocker is more of a hindrance to my running and cycling than the atrial fibrillation alone had been – but then again, because of the atrial fibrillation my heart function is gradually diminishing.
I should say, on a positive note, that the beta blocker is working, and is doing what it is supposed to do. I check my heart rate and blood pressure at least once per day and since I started the carvedilol I am right where the cardiologist wants me to be. And I can understand why people who aren’t trying to be athletes might like the med – it seems to have a mild calming effect. Furthermore I no longer feel like my heart is a fish flopping around in my chest, and my post work out blood pressure and heart rate has stabilized.
I am optimistic that the carvedilol will be worthwhile and will help me preserve and regain my ejection fraction. But really, what choice do I have?
So here is how things have changed so far (compared to just permanent a fib without the beta blocker):
1.) As far as mountain and road biking is concerned I have been able to ride all the hills that I used to be able to ride, although I am much slower. My wife now has to wait for me at the top of a climb, and that’s fine. I am delighted I can still ride and don’t have to get off and walk my bike.
2.) Running is more negatively influenced. My previous slow pace is even worse, and hills are quite difficult. Not surprisingly I do not like this one bit. A slow jog feels like a 5K effort. But I am still able to run – Yay!
3.) Long runs in heat are not possible. I am just not able to do a long run in heat, and lately every day has been warm. Understand that I am a big red-faced Irish-American who considers anything over sixty degrees to be hot running weather; plus I live in a very sunny place, a high desert climate without a lot of shade. It is not surprising that this is happening. A normal person running in heat will have a higher heart rate for a given pace, and will need to slow down. If you are on a beta blocker that reduces the maximum heart rate by a significant amount, well: “game over.”
My goal is to continue running and mountain biking on trails like this: Brown Mountain Trail
4.) I suspect that the beta blocker might be making me lazy. I don’t know if that is the right word, but I had a full day off in the middle of the week a while ago and I had planned on, among other things, writing this article and going for a trail run, and next thing I knew it was late afternoon and I hadn’t done a thing. What? By that time there was a thunderstorm so I was not going out for a run – but the article still hadn’t been started. I hope this is not going to be the case from now on. Being lazy and depressed is far from my idea of fun.
I am going to wait until I have had more experience with the beta blocker and write a better informed article. I’m going to sign up for a relatively flat (downhill, actually) trail half marathon and try to redeem myself.
In the meantime I would love hear about other people’s experiences with the dreaded beta blockers. Please post a comment below.
One of the nice things about endurance sports, from half marathon and up, is that most participants do not have this type of attitude. It is a live and let live culture. It seems like half marathons in particular are a plce where you generally see conspicuously non-athletic looking athletes – and good for them!
Half Marathon Participant – Right on!
As for me, I’m in permanent atrial fibrillation, which makes me slow, and now I have to take a beta blocker, which makes me even slower.
But I’m certainly not going to stay home, and I’m going to remain a trail runner, even if I’m slow, and I still plan on signing up for distance events. At my last half marathon I was very surprised to see almost the entire field, including people who would previously never had been in front of me, pass me, get smaller, and disappear from sight. In the first two miles. Not fun. I was thinking, “Whoa, where’d everybody go?”
Contrary to how it might appear to faster runners who are observing slower runners, it’s not always easy being slow. It might actually be more difficult. Yesterday on a four mile trail run, my first run on the beta blockers (more on that later), I rounded a corner and saw another runner behind me. He was an individual who I had seen at the trailhead, who appeared to be a bit older than me, and who was wearing jeans and a long sleeved shirt on a ninety degree day. I thought, “Oh man, I don’t want to get passed!” and I cranked up my speed. I don’t think I was running fast at all, maybe about a ten minute mile, but the burning in my lungs and legs felt like a fast 5K. “This is ridiculous!” I thought, saddened. This is “fast” for me now.
But that is my new reality.
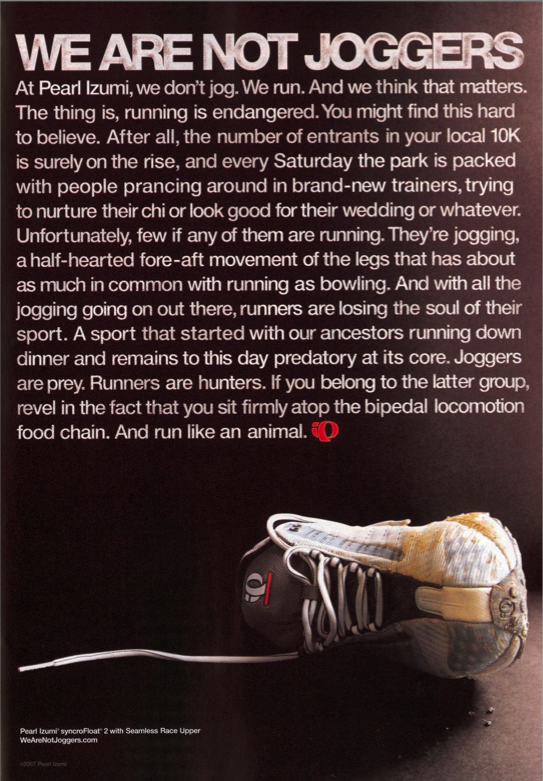
As far as Pearl Izumi is concerned they evidently think that being assholes, and creating some controversy, will make their ads stand out. They may be correct. There are a lot of competitors out there, they have an extremely small market share, and it is said there is no such thing as “bad publicity.” I knew that they made shirts, and jackets; but until now I didn’t even know they sold shoes.
Pearl Izumi Shoes – so fast you’ll kill your dog!
One of their ads last year, which featured a runner who ran so fast in his new Pearl Izumi shoes that he killed his dog, made quite an impression. Of course they apologized and had their (unfunny) ad featured in news stories and blogs for weeks.
By the way, my main nylon running jacket is made by Pearl Izumi. I like it, it’s a good jacket. I’m not going to boycott them or burn the jacket, or anything like that. I just want to say in this blog that slow runners are probably slow for a reason – and that reason isn’t necessarily poor character or laziness.
Me – Lazy jogger with atrial fibrillation after a twenty mile training run. I ran so slow that my dog survived!
Or even if the slow runner does have poor character, or is lazy, well, what’s it to you?
And guess what – Pearl Izumi got three of their ads posted in my little blog (and elsewhere) – for free!
Is distance running therapeutic? Is mountain biking addictive? Is there such thing as a good addiction? If my atrial fibrillation worsens and I could no longer do long runs or bike rides – how hard would it be to kick the habit?
High Lakes Trail – Southern Oregon
Today in the hospital lounge, while I was eating some potato chips, somebody was telling me how bad potato chips are for me. Whatever – I have given up almost everything in the world that is bad for me. I haven’t drank alcohol in several years, haven’t smoked a cigarette in decades, gave up meat and eggs a couple of years ago, I’m almost dairy free, and I haven’t taken recreational drugs since high school in the seventies. Potato chips, which I feel are good enough to be “worth it,” are about it for me. Well, that and diet soda, which is also an unhealthy habit that I have.
But what about “runner’s high?” Is that my addiction?
And what exactly is runner’s high? Does it even exist? I’ve been hearing about it for a long time, even before I started running in the early 80s.
Allegedly the athlete’s brain is “flooded with endorphins, more powerful than any street drugs!”
Many distance runners claim to experience euphoria during or after running, and some claim they’ve never had it happen – not even once.
The endorphin theory is the oldest, but more recently I’ve read about how endocannabinoids (naturally occurring neurochemicals related, in a way, to the active ingredient in cannabis) might be the cause of runner’s high.
Whatever the cause, it certainly appears to be real.
Pacific Crest Trail via Brown Mountain Trail – Klamath County, Oregon
Ultrarunner Dean Karnazes describes the role that running has in his life: “Some seek the comfort of their therapist’s office, other head to the corner pub and dive into a pint, but I chose running as my therapy”
“I’m convinced that a lot of people run ultramarathons for the same reason they take mood-altering drugs. I don’t mean to minimize the gifts of friendship, achievement, and closeness to nature that I’ve received in my running carer. But the longer and farther I ran, the more I realized that what I was often chasing was a state of mind – a place where worries that seemed monumental melted away, where the beauty and timelessness of the universe, of the present moment, came into sharp focus.”
― Scott Jurek, Eat and Run: My Unlikely Journey to Ultramarathon Greatness
Actually, a recent New York Times article states that on good experimental evidence it has been finally determined that exercise does indeed produce a flood of endorphins in the brain. Lucky us!
Researchers in Germany, using advances in neuroscience, report in the current issue of the journal Cerebral Cortex that the folk belief is true: Running does elicit a flood of endorphins in the brain. The endorphins are associated with mood changes, and the more endorphins a runner’s body pumps out, the greater the effect.
I won’t review the article here, but please read it – an elegant experiment, and solid conclusions.
But irrespective of the cause, what is runner’s high and what does it mean to endurance athletes? Can a person become addicted to it?
Personally I feel that the term runner’s “high” is a misnomer. I would describe it better as an altered state of consciousness rather than a high. Maybe I’m splitting hairs but I have never felt intoxicated by endurance sports.
Euphoria might even be too strong of a term – but maybe not. There are times during and after running when everything appears exceptionally crisp and beautiful. That’s why I love trail running, in Oregon, in the wilderness – does that happen to people in health clubs running on treadmills?
After an hour or so even carb gels seem remarkably delicious!
Also – music becomes intensely enjoyable. I do run with an iPod and sometimes I feel I am going back to the days back in high school when I smoked pot and would listen, chemically enhanced, to suddenly amazing music on headphones. Except now instead of sitting in a darkened basement I’m moving through the woods. It’s funny – a lot of the music that, for me, is most enjoyable on long runs, is the same type of music that I believe would be most enjoyable to a person who is stoned. Sometimes a song sounds so good I’ll repeat play a song two or three times.
But another reason I don’t like the title “runner’s high” is it isn’t all euphoria, beauty, and music joy. I think the exercise induced altered state of consciousness can involve a certain amount of emotional lability. Here’s an example: once I was on a twenty mile trail run, and at mile sixteen an old song I hadn’t heard in years, Careful With That Axe, Eugene, started playing in my random shuffle. This very early, nine minute long Pink Floyd song is sort of a novelty song; a one chord song that slowly builds on a rising and falling bass line with a mellow organ playing over it. At one point a whispering voice says, “Careful with that axe, Eu-zhene.” And then there is this horrific screaming and dissonant guitar, and finally it evolves back to the mellow bass and organ. Back when I was in high school, if we had somebody over who had never heard the song before, we’d put it on and turn down the lights, and of course when the screaming began it would scare the crap out of the first time listener, and we’d all have a good laugh.
Well I knew all about what was going to happen during that song and wondered if I would start laughing when the “axe” section came up. Imagine my surprise when I burst into blubbering tears when the screaming began. I should state that this was shortly after my ex-wife (with whom I was still friendly) and her family had died in a horrible house fire – but honestly I wasn’t even thinking about that until the screaming in the song. I know I wouldn’t have been anywhere near that emotional if I hadn’t just put in sixteen hilly trail miles.
Other times while running something will strike me as funny I will begin laughing giddily – out there all by myself, or in the back of the pack at a marathon. Or an angry song will play and I’ll feel, like, GRRRRRRR!, become angry – quite a catharsis.
GRRRRRRRR!
So is exercise induced altered state of consciousness addictive? I’m thinking: yes.
C – Have you ever felt you needed to cut down on your running? A – Has anybody ever annoyed you or criticized your running? G – Have you ever felt guilty about your running? E – Have you ever felt you needed a run first thing in the morning (Eye-opener) to steady your nerves?
Well – I can honestly say I’ve never felt guilty about my running, but the rest of those questions, well . . . .
And I can state for the record that with my atrial fibrillation, and the likely progression of my a fib, including my upcoming need to be on a beta-blocker, I have been dreading the day when I am no longer able to run. Very depressing.
Biking in A Fib – like riding through mud
Aside from that I have a theory. I think it is obvious that not everybody will experience anything like a runner’s high. Clearly many people hate the way running makes them feel, and they are the people who think distance runners are completely nuts. And why wouldn’t they? Based on the time they ran two miles and felt nothing but fatigue and pain, and interpolating that up to, say, thirty-one miles, their obvious conclusion would be “WTF?” to use the parlance of our times.
Lyon’s Trail – Lava Beds National Monument
But as for myself, and I’m guessing most of the people who would be interested in this blog, the so-called runners high can be generally considered to be a gift.
Diversion: How to talk to your children about distance running:
Hyponatremia (low sodium, or “water intoxication”) is a risk for runners with atrial fibrillation. It is certainly a risk for me and I believe I have experienced it a number of times in the past. Personally, I am much bigger than most marathoners (6’3” 205 lbs), and because of that and the atrial fibrillation, much slower – so I’m out there twice as long and sweating twice as much. Plus – over the years it has been drilled into all of us to make sure we drink enough water.
Ironman athletes, ultrarunners, and bigger runners are all at increased risk because we are simply out there for much longer periods of time. Women athletes tend to be at higher risk for hyponatremia – it has been found that women hydrate more during a race.
Drinking enough water is a good idea – but it needs to be accompanied by increasing salt intake.
Normal levels of sodium are about 135-145 mEq/L. Symptoms are likely to begin at 130 or lower and if you get below 120 the condition may become fatal. While there are a number of medical causes for hyponatremia marathon runners fall into the category of consuming too much water and not enough sodium, and sweating out valuable sodium. Think of the white dried salt on your temple or on your hydration pack straps after a long run.
Symptoms include bloating, headache, swelling (check to see if your ring or wristwatch seems to be getting tight), nausea, vomiting and eventually weakness, restlessness, confusion, and well . . . it just gets worse from there. It is particularly problematic for runners because some of the symptoms (headache, nausea, cramps, and dizziness) are the same symptoms for dehydration so the impulse is to drink more water – which of course makes it worse.
There is currently an ongoing study at the Houston Marathon involving volunteers who are followed closely, weighed, fluid intake measured, lab studies obtained, etc. The study found that runners with lowered sodium levels drank more water, retained more water than normal volunteers, and they lost more total sodium and had saltier sweat.
Runners who were dehydrated but not hyponatremic had higher heart and respiratory rates, felt worse, and had lower blood pressure than hyponatremic runners. The hyponatremic runners felt better, but had more nausea and bloating.
What can be done?
Drinking less water is sometimes recommended but it is difficult to do when you are used to drinking a lot of water while running. I’ve tried drinking less water during a marathon and frankly I think it made things worse. Also some runners can become hyponatremic without over-doing the water consumption.
Weighing yourself frequently along the course and looking for weight gain (water retention) has been recommended – YEAH RIGHT! How is this going to happen?
Personally I try to drink water with sodium supplemented (NUUN, GU Brew), and try grabbing some little pretzels at aid stations (if available); but some research suggests this might not always be helpful.
Fatigue? Really? Fatigue during a marathon – you don’t say? Isn’t that generally a part of the experience?
I don’t have a good answer. I know I’ve had problems with this – I’m clearly in the high risk category for hyponatremia. I also generally have particularly poor races if it is a warm day.
My interventions include
1.) Drinking enough water
2.) Electrolyte supplements in my water (NUUN, Gu Brew)
3.) Additional electrolyte supplementation (SaltStick caps, Endurolytes caps, little pretzels)
4.) Making sure I have a salty snack or meal after a race or long run
5.) Trying to dress so I’m a little cool rather than a little warm
I’d love to read your suggestions – please leave a comment if you have any experience with hyponatremia and suggestions as to how to avoid it.
Most medical scientific organizations recommend low or moderate sodium diets to the general population in order to reduce the risk of high
blood pressure (hypertension).
Regular physical activity reduces the risk of hypertension.
Athletes lose sodium in sweat during exercise. The amount of sodium that is lost during endurance exercise depends on the sweating rate and
the concentration of sodium in the sweat. In turn, sodium loss during exercise depends on individual factors, such as genetics, fitness and heat
acclimatization, as well as the type, intensity and duration of exercise and the external environment.
Sodium ingestion by endurance athletes does not typically increase blood pressure, so low sodium diets are not recommended for individuals
who participate in long-term aerobic exercise.
Sodium ingestion during or following endurance exercise will help to stimulate thirst and drinking as well as stimulate fluid retention by the kidney.
No athletes are immune to hypertension, so athletes should monitor their blood pressure as they do their general health. This is particularly
important for older athletes, athletes with a genetic predisposition to hypertension, stroke or other cardiovascular disease.
I’ve signed up for a Spring marathon – specifically the Vernonia Marathon. It is in Northern Oregon – North and West of Portland – a part of the state that I have never visited. I think this might be my 18th or 19th marathon but I’m not sure.
I just did my first true long run and I feel pretty good. I informally classify runs like this: two to six miles are shorter runs, like mid-week type runs. Medium long runs are nine to twelve miles. I’ll usually try to do a nine to twelve mile run every weekend even if I’m not training for anything. In fact, if I’m not training for anything at all sometimes that’s my only run of the week (with mountain biking or hiking on other days). I think of a true long run as being fourteen miles and up. There’s something about that distance that, for me, seems pretty serious. Anything over thirteen requires more fortitude.
I didn’t just start training for an April marathon this weekend – I’ve been training for weeks – but my weekend long runs have only been eleven to twelve miles.
As far as my atrial fibrillation is concerned nothing has changed – I remain in atrial fibrillation all the time, my running has slowed, and I need to make sure I drink enough water and eat something salty afterwards. After the fourteen miler I went through the drive through at Burger King and bought each of the dogs a cheap burger from the value menu (the dogs aren’t vegan), and just an order of fries (with salt) for me. This way I avoid the dizziness I sometimes get from standing up after a long run.
Sophie Tired After a Long Run
The Vernonia Marathon course is on a paved bike trail. This is the first Rails to Trails project in Oregon – the OC&E Woods Line State Trail being the second. I chose it because I like to train on the OC&E and have completed the Bizz Johnson Marathon (on an un-paved rail trail) seven times.
Sophie on Paved Portion of the OC&E Trail
I dislike running on pavement so hopefully there will be a dirt trail off to the side of the paved part. If not – well, a paved trail seems a lot softer because it is simply pavement on top of gravel as opposed to pavement on top of concrete (which is what our local streets are.)
I expect the Vernonia Marathon should be a small, informal, fun race and I won’t know anybody there except for my friend Claude who is also going to run it.
Winter Training
My race strategy is to start out slow and then take it easy. The course profile looks hilly – but how steep can a rail trail be? Trains can’t go up more than a one or two percent grade, right? I think the hills will be gradual – like the Bizz Johnson course.
Funny – I always enjoy the training much more than the actual races.
If anybody has any experience with this event please comment below. See you there.
I saw this link today on Facebook and thought I would share it – it is an AF Stroke Risk Calculator, and was posted by the Atrial Fibrillation Association – a great resource for people with atrial fibrillation. As you probably know one of the greatest risks of being afflicted with atrial fibrillation is that it can lead to you having a stroke. Blood clots can form in the malfunctioning atrium, break loose, travel to the brain and – BOOM!!!! – you’ve had a stroke. Prevention is the best approach.
This calculator is basically a clever automated version of the CHADS2 score. I was delighted to find my risk is 0%.
But if course my risk is definitely higher than zero percent – even if my CHADS2 score is zero.
My heart is abnormal in more ways than the atrial fibrillation. I have hypertrophy of my left ventricle (from running – not a risk factor) but I also have “severe hypertrophy” of my left atrium (the top chamber of the heart) which my cardiologist assures me is a risk factor for stroke and although my CHADS2 remains zero I am on an anticoagulant (Pradaxa).
My question has been: Why not include left atrial hypertrophy in the CHADS2 calculation?
Answer: I dunno.
Lillian and Lolawanda ready for another trail run
My other question has been: What else can I do to reduce my risk of a stroke?
I understand my risk is NOT zero, regardless of what this calculator says.
Obviously one thing I know I can do is to remember to take my Pradaxa twice daily. Believe me, for somebody who is only taking one medication it isn’t as easy to remember as you might think. I have considered switching to Xarelto simply because of the once a day dosing.
My Pradaxa
But other than that what else can I do? One more thing (I think) – stay well hydrated.
As a large, slow, long distance runner (who is often on the trail for several hours at a time) I sweat more than smaller runners, and I have to be very careful not to become dehydrated. I spoke with a friend of mine who is an Internists/hospitalist and he agreed – don’t become dehydrated. Being dehydrated can literally thicken the blood and increase the chance on a clot, and therefore increase the chance of a stroke.
Be Careful Out There!
How much water should a person drink? I have no specific prescription but what I do is try to drink enough so that my urine is relatively clear once per day. Also there is such a thing as too much water and big, middle-aged distance runners are at relatively high risk of hyponatremia (too much water – not enough sodium) so be careful out there!
We talked about other risk factors are there? Risk factors for blood clots in the legs include being inactive, obesity, and smoking – probably less likely for the readers of this blog.
Sedentary after a LONG RUN
What about alcohol? Does that increase the risk? He said probably not and in moderation might even decrease the risk – but remember – alcohol clearly increases your risk of atrial fibrillation – and if you drink enough alcohol you will become dehydrated – so there you go!
By the way – don’t expect this this risk calculator or this blog to advise you as to whether or not you should take your aspirin, your warfarin (Coumadin), your Xarelto, or your Pradaxa. It is important that you make this decision with your doctor.
The thing I enjoy most about the afibrunner blog is comments from other athletes who are dealing with atrial fibrillation. A recent comment from a runner (we’ll call him “Lon”) really caught my attention – here is a runner who, while in atrial fibrillation, was able to race at six minute mile pace (or better).
Here are some excerpts from his comments:
Way to Go!!!
Since 1983 I’ve run/jogged 59 full marathons and have suffered with A-fib on and off for the last 12 years. I’ve finished the Boston (2001 in 3:23) and NY City (2005 in 4:15) marathons while in constant A-fib while carefully monitoring my heart rate. My cardiologists encouraged me to run marathons and also triathlons. One cardiologist told me that my heart is so strong that it laughs at A-fib and that I have the heart of an olympic cyclist. For the first 6 months of this year my heart was in constant A-fib that no drugs or multiple cardioversions could put it back into normal sinus rhythm. On July 9, 2013 I had the “Wolf Mini-Maze” (at the International A-fib Center of Excellence in Indianapolis) operation done on my heart. It was a great success and my heart has been in constant normal rhythm ever since (nearly 6 months now and I’m not taking any medications). In the Mini-Maze they removed my Left Atrial Appendage (LAA) so that if my heart ever goes back into constant A-fib I will NOT meed anticoagulant therapy. As you likely know life threatening blood clots tend to form in the LAA when your heart is in constant A-fib. The risk of stroke over the life time of an A-fib patient is huge. 3 out of 5 A-fib patients will suffer a stroke in their life even while taking anticoagulation meds like coumadin. That is a statistic that your doctor will not likely tell you about. Coumadin is over rated and is simply not very effective for some people which should be a terrifying realization to anyone dealing with A-fib. Anyway, as much as I love marathons, I’m laying off the long distance jogging for a while and am just jogging 10K’s (one per moth and 3 sprint triathlons this Summer) as well as several other physical activities.
Good health to you!
Lon
I have lamented that atrial fibrillation has made me slow, while openly admitting that I started out slow – I’ve only ran, as far as I know, one six minute mile in my entire life – and that was thirty years ago.
Finish Line – Eugene Marathon
My understanding about atrial fibrillation is that the atria no longer preload the ventricles, and most people have a decrease of about 20% of their cardiac output. While sedentary people might not even notice this athletes certainly would. I do!
But I have heard that in some patients, certain athletes, there is little change in cardiac output and atrial fibrillation will not affect performance much. Lon seems like one of these fortunate people. Lon’s point about the increased risk of stroke (even if you take your Coumadin, Pradaxa, or Xarelto) is well taken – and I’m guessing that that is why he continued to pursue an effective treatment for his atrial fibrillation.
Finish Line – Haulin’ Aspen Marathon
But after all those marathons Lon states he is no longer running endurance events – he goes on to elaborate:
Here’s a little more. I tried not to make a long story short above. I left out mentioning that I had a radio-frequency catheter ablation in June 2010 in Seattle that worked great in keeping my heart in normal rhythm until December 2012 when suddenly for no apparent reason went into persistent A-fib. (During that 2 1/2 year period I finished 9 full marathons and 8 sprint triathlons) My heart stayed in persistent A-fib even after 4 cardioversions and large doses of amiodarone. My cardiologists in Seattle told me that I should accept my persistent A-fib and they offered to ablate my hearts pace makers (AV and SA nodes) and give me an electronic pacemaker so that my heart rate can be controlled. That told me that I needed a second opinion so I started communications with Dr. Randall Wolf in Indianapolis about his Mini-Maze procedure. After consultations with an E.D. doctor (and a championship Iron Man triathlete) who had the Mini-maze operation and was very happy with the results, I decided to get the Wolf Mini-Maze and of course I informed my Seattle cardiologists of my intentions and they said to go for it. Absolutely the main reason that I went for the Wolf Mini-Maze is that it removes the left atrial appendage which brings my risk of stroke down to that of a healthy person with a normal healthy heart while not taking any anticoagulation drugs. The fact that I now enjoy a normal heart beat is just a huge plus factor.
From 1983 until December 2012 I completed 61 full marathons a most of which ran with all out efforts (I’ve averaged sub-6 minute pace all the way). I’m now finding out that long distance running is simply not good for the heart and most likely caused my A-fib problem.
Google Dr. John Mandrola’s 18 minute video called “Cycling Wed: I told you so…”. It is very illuminating and a must see for all endurance athletes. Please check that out.
Cordially,
Lon
I don’t know much about the Wolf Mini-Maze procedure and don’t necessarily advocate it for everybody, but clearly it worked in Lon’s specific situation. Here is some information regarding the Wolf Mini-Maze.
Finish Line – Lake of the Woods 15K
No need to Google the video by Dr O’Keefe (posted on Dr Mandrola’s blog) I have the link right HERE.
Here’s the video:
If you don’t feel like watching the eighteen minute video I will summarize it for you – Exercise is good for you but in moderation. Too much or too intense exercise causes chronic inflammation of the heart and can ultimately harm the heart (atrial fibrillation, among other risks).
But if you are an endurance athlete dealing with atrial fibrillation you already know this – surely you have had a dozen or so friends and relatives, possibly sedentary and/or obese, kindly forward you information about the study he refers to – as if to justify their seemingly wise choice to avoid marathons and triathlons and replace it by watching other people play sports on television. Yes, this study was in all the newspapers and magazines last year.
Finish Line – Avenue of the Giants Marathon
Please understand, and I paraphrase here, that Dr O’Keefe states that exercise is good for your heart, and being obese and sedentary is bad for your heart – but that overdoing it is a problem. He didn’t say people should avoid exercising.
My choice – I understand the concept of the “law of diminishing returns” as well as the next guy; but for me, well, I enjoy long, slow trail runs and mountain bike rides more than just about anything else I can think of – so I chose to continue.
Finish Line – Bizz Johnson 50K (I completed the 50K in atrial fibrillation)
This year, October 13, 2013, was my seventh time running the Bizz Johnson Trail Marathon. My first time was in 2007 and I have ran the event every year since then. Last year I ran the 50K (31 miles), but it is pretty much the same course, just 5 miles longer.
Has anybody reading this blog knows I have been in persistent atrial fibrillation for the last two years. For the 50K last year, and the marathon this year, I was in known atrial fibrillation. I am pretty sure that I went into atrial fibrillation about two thirds of the way through the 2011 marathon. At least (in retrospect) it felt that way, but that was before I knew I was afflicted with this dysrhythmia.
It took a long time to get to the finish line this year
The course of the Bizz Johnson Trail Marathon is well known to me and I enjoy it a great deal. The Bizz Johnson Trail is a rails to trails project, and is about 24 ½ miles long. For that reason the race begins with an out and back on a Forest Service fire road in order to make the marathon and official 26.2 mile run. Once the runners get on the actual rail trail the course is a gentle uphill until about the 6 mile marker at which point there is a 20 mile downhill section. This might sound like it’s easy, but remember, it’s a run not a bike ride. This is the only race where afterward I typically have a lot of quadriceps and heel pain from all the downhill.
Except for the portion where the trail crosses the Susan River Canyon the grade is very gradual. Trains evidently are unable to go up or down anything that is too steep, and the average grade is below 1%, and at its steepest probably about 2%. This is an estimate, I’m really not sure of the exact grade. One thing I can say, though, is that the steepest downhill is the last 6 miles down the Susan River Canyon. This is also where the course is the most scenic (including two tunnels) and often this section is quite warm.
This year the deciduous trees were changing and it was quite beautiful.
Along the course (No deciduous trees here – sorry)
Some people worry about the elevation at Bizz Johnson, but to me that isn’t even a factor. I live and train at the exact same elevation as the Bizz Johnson Trail. As a matter of fact I do almost all my training on mountain biking and hiking trails which are much steeper and more technical than the Bizz Johnson Trail.
I have to admit I had a bad time this year. I don’t think it had anything to do with the atrial fibrillation per se, I think I worked myself into a bad attitude, or bad mental state this year – ruminating over certain past events on the two and a half hour drive to Susanville the day before the race. Also I had trained for the 50K, but I really didn’t feel up to it and the day before the race I switched to the regular marathon. This probably was a good move, but I felt somehow depressed over that choice.
I’m not sure how many marathons I have ran, but it’s somewhere between seventeen and twenty races. There comes a time in every marathon where I start to feel poorly, but usually I don’t start to feel that way until somewhere around mile twenty-two or twenty-three. For some reason at this year’s Bizz Johnson I started to feel that way about mile six. “It’s going to be a long day,” I told myself.
Ultimately I completed it, I suffered like an animal, but I lived to fight another day. It’s interesting that I finished it at almost the same time that I finished the 50K last year, that is taking into consideration that the 50K starts an hour before the regular marathon. My recollection of the 50K last year is that I felt much better, surprisingly, throughout the entire race than I have during any previous marathons. Maybe I should stick with 50Ks.
My friend Stephen, who ran the race this year as well, said he suffered like an animal as well, and that “it seemed like every mile hurt.” But then again he finished several hours ahead of me, came in seventh place overall, and won his age group. It was probably worth it.
Sometimes I wonder – am I good at marathons? Maybe. Maybe not. I’m certainly not fast. Seems like I did a good job, the night before, sitting in a motel room watching sitcoms. Maybe I’m better at something like that. Well, I guess I’ll have to keep trying marathons until I get one right.
Finishing the 50K last year
Being a veteran trail runner who has to be self-reliant, except during a race, I carry my own water. I use an Ultimate Design WASP hydration vest, with NUUN tablets added for electrolytes. I refill it at the water stops if necessary. This year, for some reason, I figured I should probably drink some of the electrolyte drink that they offered at the water stops in addition to my own concoction. I should have known better. It was a pink drink that is evidently marketed by the Power Bar company. I have never tasted a urinal cookie before, but I imagine that this pink sports drink is pretty close. Every time I drank a Dixie cup of it at a water stop I had to walk a little bit and try to hold it down. In other words I was having a lot of nausea. Being nauseous will not prevent me from drinking because I figure I can always drink more water if I vomit, but it sure does keep me from eating, so I was a little deficient as far as carbo gels were concerned. I think I only had two all day (and had planned on five).
During last Sunday’s race I decided that the mile between mile marker twenty-three and mile marker twenty-four is definitely the cruelest mile. Suffering is maximized, and you’re close but not really close enough to the finish. If I tell myself, “it’s only three more miles!” I then start to think that three miles sounds like a terribly long distance.
I enjoy listening to music on my iPod shuffle while I run and when I arrived at the last quarter mile of the race a terrific song came on my iPod. It was Oh Comely by Neutral Milk Hotel. Unfortunately I was feeling remarkably emotionally labile at that point in time that I knew that if I listened to the song I would start crying. I already knew I was suffering and wasn’t going to appear well coming across the finish line, but I really didn’t want to finish crying like a little kid – so I fast forwarded it. I clicked until I found a song that was a little bit more emotionally bland.
When the finish line mercifully appeared I was glad to be done. I strolled over to the feed section and as usual there were a lot of great things to eat, but I was feeling so nauseous – there was not one thing there that I could’ve eaten. Claude, who also ran the race that day, was waiting for me and we took the shuttle back to the parking area. I had some food in my truck for post race meal, but as soon as I walked over there I became quite sick and expelled a large quantity of pink water. It must have just sat there in my stomach – there was a lot of it! I felt much better, changed into my dry clothes, and ate my post race meal. I started to wonder – emotionally labile, tearful, and nauseous – was I pregnant? (Ha ha)
One big difference between running in persistent atrial fibrillation and normal sinus rhythm is that, for me anyway, there is a lot of apprehension about over-doing it. The days of charging up a hill may be behind me at this point, and I haven’t done anything resembling a speed work-out in well over a year.
Prior to atrial fibrillation I used to do interval work-outs once in a while. For certain marathons where I had a specific personal time goal I would do a work-out known as “Yasso 800s.” Although some expert dispute that this is actually the most effective speed work-out for marathon training, nobody would dispute that this is a difficult work-out. I would do them on Wednesday nights at a local college track and I always felt they were my most difficult work-out of the week – probably more challenging than my languorous week-end long runs. Certainly this was the work-out where most feared injury.
To be honest I don’t miss Yasso 800s. I never have been a fast runner and never enjoyed short fast races like 5Ks.
But even during LSD (long slow distance) work-outs there usually comes a point where I will feel that the run is becoming difficult and I have to push through that. People often say “push through the pain,” but it isn’t really “pain” per se; but whatever it is it now makes me nervous!
But now that I am in persistent atrial fibrillation I think twice about pushing beyond any thresholds, however they are described. I have a fear in the back of my mind that I am going to make the atrial fibrillation worse, or pass out, or die, or . . . well who knows? This is all new territory for me.
I think this is why I “bonked out” of the second and third (out of seven planned) twenty mile runs I did during my build-up to this Sunday’s Bizz Johnson 50K. I just wasn’t willing to risk it. But if I’m unwilling to risk it it is obvious that I will only get slower and slower each year.
RINGO SAYS RELAX
I’d love to hear from other endurance athletes about this topic whether you are in a fib or not, and whether you are risk averse or not. Please feel free to leave a comment.