I haven’t blogged for a while because we’ve been on vacation in Croatia for two and a half weeks, and of course after being gone for that long I’ve been incredibly busy at work. I am working on along blog entry (actually it’ll be a separate blog) about Croatia, so stay tuned.

Me During a Brief Rest Stop
In my opinion bicycling around Crater Lake is one of the finest bike rides in the entire United States, and Crater Lake National Park will, from time to time, close of twenty-four of the thirty-three miles of the Rim Drive to allow bicyclists, hikers, and runners to have a relatively car free day. This year they had vehicle free days on two Saturdays: September 20 and 27, and I made time to be there for both days.
Since I live near Crater Lake N. P. I’ve had the opportunity to ride the rim several times, but this year was my first time doing it in permanent atrial fibrillation (and while on a beta blocker). Always a challenging ride under any circumstances, adding a fib and a beta blocker to mix changes things a bit.
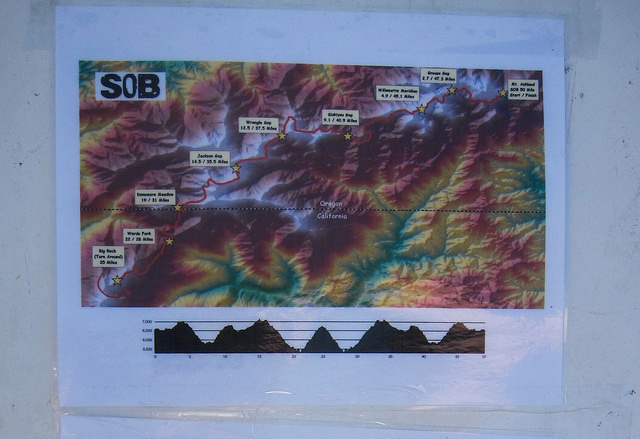
Most riders start at the Steel Visitors Center (Park Headquarters) and ride clockwise. The first thing on the agenda is a three mile climb with 650 feet of elevation gain up to the Rim Village. This is actually the steepest hill along the route, but not the most difficult, in my opinion, mostly because the legs are still fresh. It is quite odd to pedal up a climb like that and find a lake at the top. There are several climbs and descents along the thirty-three mile route, and rarely is there any flat road, and the two toughest climbs, in my experience, are in the second half of the ride – the long easy climb to Cloud Cap (where most people stop to sigh and eat their Clif Bar) and the last grind up to Dutton Ridge. I might even say that you only need two gears to ride the rim – whatever you use as your easiest climbing gear and a big gear for coasting downhill.
Elevation varies from 6700 to 7700 above sea level. Personally I don’t have an issue with the elevation at Crater Lake because I’m used to living at higher elevation, but people coming from sea level might feel it.

Bicycling in Croatia with Margo
To be honest, none of the climbs (going clockwise) are particularly steep, and there is only a total of about 3500 feet of climbing, but the climbs are so long and persistent that it seems like more. The descents can be fast and one could easily go 50 mph down the descent from Cloud Cap, but don’t. The speed limit is 35 mph and there are often surprising potholes encountered once you get up above 40 mph. The vehicle free days are great because you don’t have to worry about cars behind you. One day I was descending at 45 mph, a speed at which the wind in my ears prevents hearing anything, riding right down the middle of the lane, and was passed by a van. I thought, “What’s your hurry, bro? I’m already going 10 mph over the speed limit!”
The scenery is world class and seeing it slowly, up close on a bike, complete with the sounds and the smells is unimaginably beautiful. Being there on a vehicle free day with hundreds of bicyclists from all over Oregon is even better – there is an amazing energy in the air on the vehicle free days.

Snowshoeing with Libo April 2013
If you are going to ride the rim, especially on a vehicle free day, keep in mind that once you are past the Visitor Center and the Rim Village (basically once you are past the first three miles) there is no water. I’m a heavy sweater so I’ll take three liters on a hot day. Actually along the last big climb there are some little “waterfalls” right along the roadside and I have seen people filling their water bottles there and it is probably fine; but it is definitely not tested and designated as potable water. Also keep in mind that there will be no SAG wagon trailing you so make sure you have the proper gear and tools for changing flat tubes and minor repairs.
As far as riding the rim in a fib while on a beta blocker, well, it is much slower. I was able to ride it but it took me at least an extra hour. I had a triple chainring on my old road bike, and I used to be able to do the entire ride in the middle chainring (except for part of the first climb); but now I am using my easiest gear for most of the climbing (my new bike has compact double, but the gearing is similar). I think I need to be happy with being able to complete the ride without falling to pieces, and quit lamenting my slower speed.

Photo by Margo
My personal preference, now that I am in a fib, is to keep going and minimize rest stops. It seems every time I stop it’s like starting over again. On the first Saturday I was riding with a group of friends, including my wife Margo (her first time doing the rim ride) and I told them I wouldn’t be stopping much and that they could catch up to me. The last I saw them was at the top of the first climb, and I actually completed the ride a half hour or so ahead of them – they had fun, stopped at the many overlooks, stopped for lunch. I was the tortoise to their hare; slogging up the hills and only stopping a few times.
Another difference is that now that I am on an anticoagulant I brake a lot on the descents. I’m usually the biggest rider in whatever group I’m riding in and consequently the slowest climber that makes up for that by being the fastest descender. No more. Now I think about how descending slowly will help me keep my blood inside my body and I was passed by dozens of riders on each hill. As a matter of fact I kept getting passed by the same groups over and over. They’d pass me on the climb, then I’d pass them at the top of each hill where they’d stop to look at the stunning view of the lake, then they’d pass me on the descent and I’d pass them again at the bottom of the hill where they’d evidently stop to chat. Over and over – sort of fun.

Skiing with Jan (evidently I’m relying on old photos because I only took one photo for two days of riding around Crater Lake – like I said I don’t stop enough!)
I returned and rode the Rim Drive again the following weekend as well but my friends didn’t accompany me. It was a much cooler, windier day and looked like rain, and they had other plans. I ended up doing the first half and deciding to make it an out and back. I was thinking about the big descent down the other side of Cloud Cap in the heavy wind and thought that might not be the best idea on account of my being anti-coagulated. I learned that riding the rim counter-clockwise is not as safe as riding clockwise. When riding clockwise the lake is to your right; but when riding counterclockwise there was quite often a steep drop off and no shoulder and no guard rail. The drop offs weren’t a thousand feet or anything like that but they were certainly much further than I wanted to go over on my bike so I did the long descents towards the middle of the lane although I pissed off a few drivers I will live to ride again. There is no way I will ever ride the entire rim counterclockwise. Keep in mind that most drivers are looking toward the lake (why wouldn’t they) and if you are between the driver and the lake they are likely to see you. But when riding the other direction there is more risk of being unseen.
Carter Lake Century 2011 (not my video)
Another good time to ride around Crater Lake in the Crater Lake Century. I have never ridden with the organized century (I’ve always been training for something at that time – it’s held in August) but I have been told it is a blast. As far as I know the Rim Drive isn’t closed during the century but there are about 300 riders up there that day. The number of applicants is limited so register early if you want to get in. The century, obviously, involves more than the thirty-three mile Rim Drive and in addition to more climbing from Fort Klamath up to the Park Headquarters, there is some routing around the local farmlands near Fort Klamath to make it an even one hundred miles.
I would love to hear from other bicyclists, especially cyclists dealing with atrial fibrillation. Please feel free to comment below.