This article is a work in progress and is only a description of my strategy for the time being. I hope to learn from readers of this blog about how to better plan for a trail debacle.

Heading out for a trail run on the Pacific Crest Trail
What kinds of things should a person like me, who is dealing with atrial fibrillation and is taking an anticoagulant (I take Pradaxa), carry on a long run in the wilderness? Or during a long mountain bike ride in remote areas?
When the high country in our local wildernesses is not covered with snow, I will generally do runs, nearly every weekend, of anywhere between six to twenty miles. I almost always run alone (except for my trail buddy – Ringo).
Dangerous and a bad idea? Possibly. But this is what I enjoy in life so I don’t plan on stopping any time soon.
The most important piece of equipment is a phone. People complain that everybody is always on their smartphone, and they should NOT be talking on their phones on mountain summits when everybody else is trying to get all Zen-like and self-actualized, and whatever – that’s a different discussion. You certainly don’t even need to have your phone on; but you absolutely should take it with you, and it should be fully charged. The days of getting hopelessly lost and spelling out SOS with rocks hoping a search plane will find you are fading into the past. A smartphone is a GPS and a direct link to help.
I always carry my iPhone in a baggie with my ID and a sheet of paper towel (which I use for unrelated toilet purposes).

Fully charged and protected from water
Even if there is poor cell phone coverage in your local high mountain or deep canyon wilderness, and a phone call isn’t always possible, I find that a text message can often still be sent. It might take a while but it eventually will be sent, especially if I am moving along a trail.
There is the standard emergency gear that most people take, often called the “ten essentials” which most people carry while in the wilderness. Of course there is truly no such thing as a standard ten essentials and the list of things you carry will vary depending on the season, your skill set, your location, and your past experience.

My generic survival gear
I got out my little survival kit that I typically carry in the wilderness, and of course not everything is pictured here, and I might not even have all of this stuff with me on any given trip. Naturally I will also have other things like food, gels, electrolytes, a jacket, and plenty of water.
What I found in my default wilderness pack is:
Two knives – a mini-leatherman tool and a standard knife. I will only actually carry one of these.
Two lights – a headlamp and a tiny LED flashlight (one is plenty).
Fire starter – a cigarette lighter, birthday candles, a tampon, and hand sanitizer (which I discovered has completely evaporated).
A space blanket, a compass.
Repair gear (Shoe laces, tenacious tape, dental floss)
Pain pills: Vicoprofen samples – okay they expired in 2000 but I’m guessing they are still good (at least for a placebo effect). Missing: Benadryl for allergies or yellow jacket stings, and I probably should have some of my Pradaxa in case I end up unexpectedly staying out overnight. Also missing: small roll of duct tape, safety pins, and my whistle!

Saint Christopher Medal
Oh, and there is a Saint Christopher medal. This one belonged to my grandfather. Well it probably won’t change anything, but it certainly couldn’t hurt. Feel free to substitute your own personal good luck charm.
But what about specific items for the runner on an anticoagulant? Is there anything else beyond the “ten essentials”?

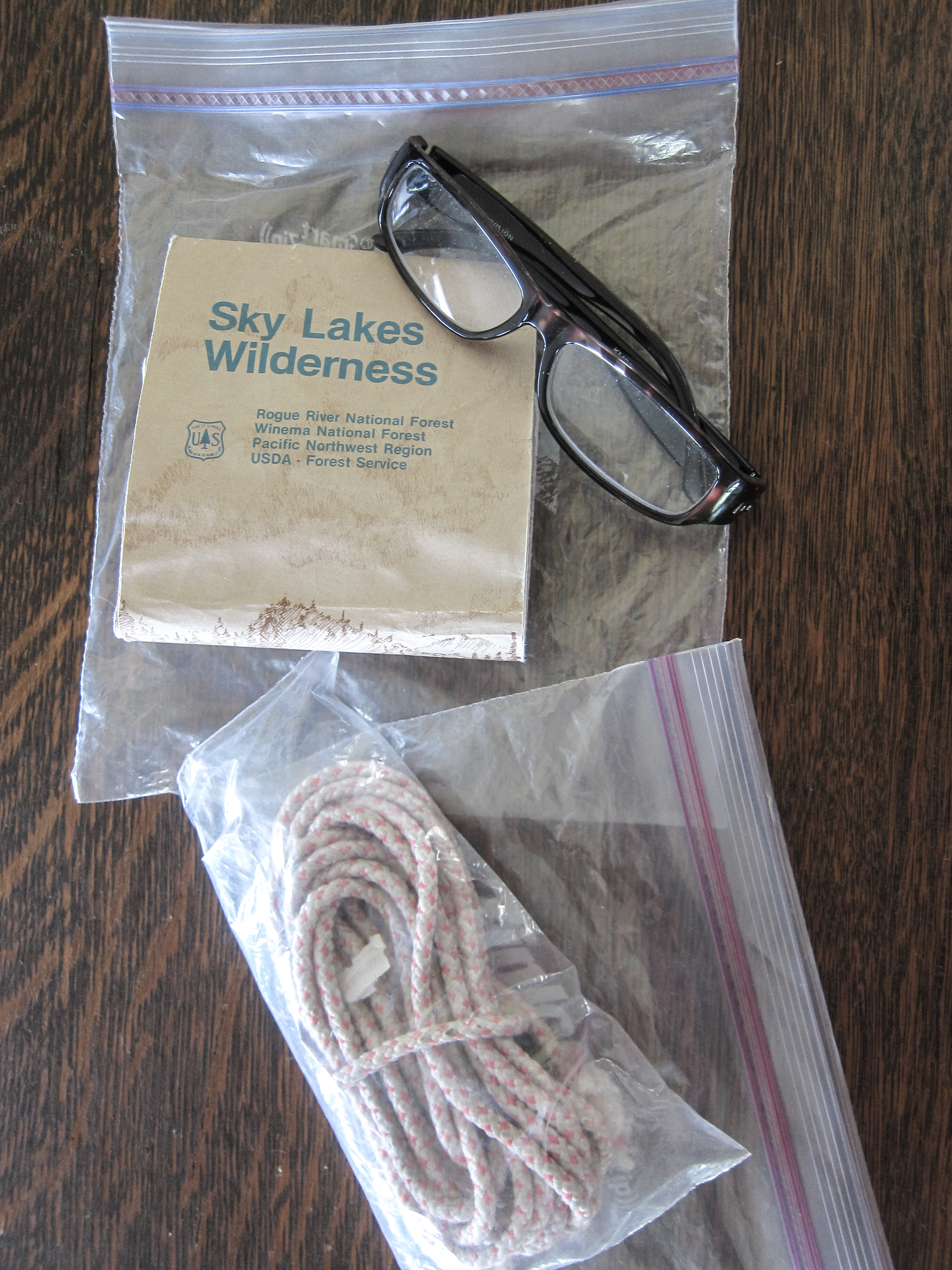
Other stuff: Map with reading glasses (if needed) and some rope
Obviously having a major bleed while running alone in the wilderness would be a disaster. Death is certainly a possibility. How can a trail runner prepare to increase the odds of a good outcome?
I always make sure to let somebody know (usually my wife) where I’m going and I also send her a text (I text “OOTW” short for “out of the woods”) when I get back to my vehicle.
I also wear a Road ID. This way if somebody finds me they will know I am on an anticoagulant. Maybe this won’t help, but it certainly is worth wearing. At least they will be able to figure out why I bled out so quickly (I know – not funny).

My Road ID
Another item I always carry is a bandanna. This can be used for a number of purposes, such as making a field dressing; but I want to have it in case I need a tourniquet. Plus – I have an extra one because my trail dog always has one draped around his neck.

Bandanna
My bandanna came in handy a week ago when my wife Margo (not on an anticoagulant) crashed her mountain bike and punctured her left thigh with her brake lever. I used it to make a compressive dressing before we road our bikes back to where we could get a ride to the hospital.
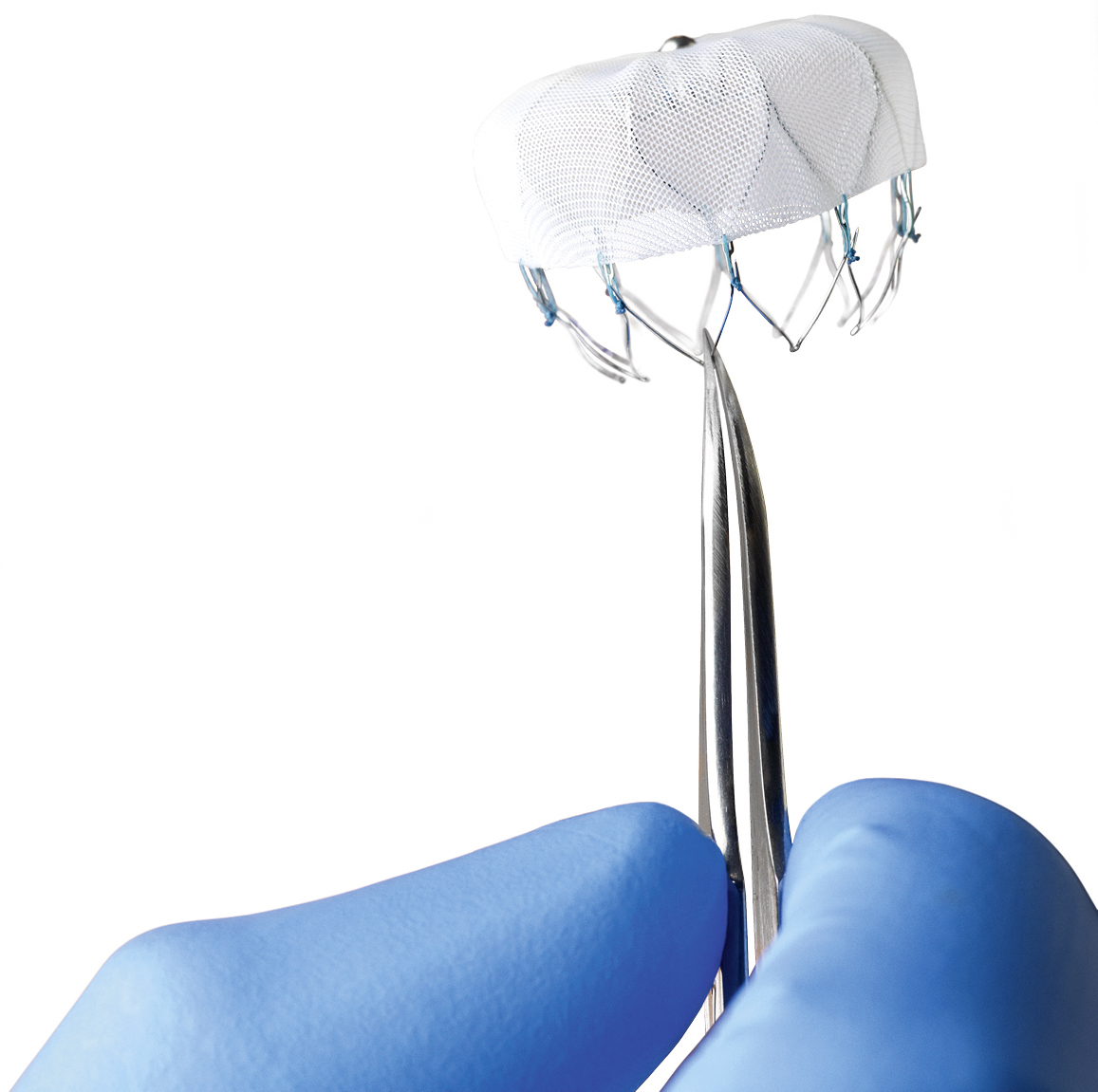
One item I do not currently have but definitely need to obtain is a Quickclot field dressing. Evidently these things really work and are routinely used in combat situations. It is a topical coagulant (an anti-anti-coagulant?) which helps clot blood and also serves as a physical barrier to bleeding. I’ve been meaning to obtain one of these for a long time. They are available online via amazon.com, and I just ordered one.

Quickclot
Question: Will the Quickclot sponge even work on bleeding in an individual who is on a direct thrombin inhibitor like Pradaxa? Answer: I have no idea. I’ll let you know if I ever get a chance to find out.
In case of bleeding the most important first step is to apply direct pressure. As a surgeon I have a lot of experience with this. Usually sixty seconds of direct thumb pressure will stop or slow most bleeding, but of course if you take an anticoagulant it will take longer. Apply direct pressure as long as necessary. Elevate the wound if possible. Don’t try to clean out major wounds as this will restart bleeding – that can be done later at the hospital.
A tourniquet is a last resort, but the bandanna can be used as a compressive dressing if needed.
Please understand that an anticoagulant doesn’t completely stop clotting of blood, it just makes it take longer. Eventually bleeding will stop. Hopefully before all the blood leaves your body!

Ringo always has a spare bandanna for me
Bonus – How to stop a nosebleed:
I have been plagued by frequent nosebleeds since I was a child but, oddly enough, I haven’t had a single nosebleed since I started Pradaxa a couple of years ago. The best method I have found is to pinch the nose, fairly tightly, just above the nostrils, and lean forward. Don’t lie with your head back – that doesn’t work. Hold for a full sixty seconds. Repeat as necessary.
If you are, like me, a trail runner or mountain biker on an anticoagulant, I would love to hear from you. Please leave comments and suggestions in the comments area below.
Thanks.