Ridgeview Trail – Moore Park
About two weeks ago I was out for my typical Saturday two hour trail run on Moore Mountain with my dogs. It was a fine day and I felt great, and with about ten minutes left in the run I ran into three of my friends who were out mountain biking. My friend Linda, a Physician Assistant, was trying out her fancy new mountain bike and we stopped to talk for a while. She showed me her new bike and I introduced her to my new dog. I noticed, and commented, that I was having a little trouble getting my mouth working properly. I didn’t have any trouble finding words, or even saying the words, but my tongue just felt sort of thick – especially with consonants like “R” that seem to be made in the back of the mouth. I immediately did my self inventory for asymmetry and muscle weakness and found none. I attributed it to having had one of those little, annoying white sores in my mouth, accompanied by some swollen glands and thought nothing of it.

Linda Cyclecross racing
I finished my run, which involved a fairly technical descent, ate my post-run Clif Bar, and went home where I noticed nothing amiss. I forgot about it until Linda texted me the following day asking how I was doing and saying she was worried about me. I assured her – I was fine!
The next Monday, at work, I thought I’d ask my friend and co-worker, Dr Zakir Ali, if he thought the incident was any reason for concern. Dr Ali is a neurologist who works a couple of days a week at the orthopedic clinic, where I work as a podiatrist.
He wasn’t as dismissive as I was about the incident and said that that was very suspicious for a TIE (transient ischemic episode). A TIE is basically a small, brief stroke, in this case likely caused by a small blood clot that resolves fairly quickly. Dr Ali said I should, at the very least, get an echocardiogram to see if there is a clot in my left atrium, and possibly a carotid artery scan as well.
I have been in permanent atrial fibrillation and on Pradaxa, a potent anticoagulant (blood thinner) for two years and had never missed a dose. I thought he may have been over reacting – and I had had an echocardiogram just two months ago.
But Dr Ali had told me, “You will never regret checking.”
And I agreed.
Okay.

So I called the on call cardiologist, explained what had happened, and he told me a standard echocardiogram would be useless as it won’t show a clot, and recommended a trans-esophageal echocardiogram, and also a carotid scan (ultrasound).
I mentioned that I had had a trans-esophageal echocardiogram before (in 1994!) and it was like swallowing a telephone. He said he’d get anesthesia involved and we set up both procedures not expecting to find anything.
So the carotid scan came first and was normal, as expected.
Last Wednesday I went to the hospital and checked in to Day Surgery – which was a peculiar and strange experience for me. I’ve been working there, as a surgeon, for the past twenty-five years, but this was my first time being there as a patient. It’s a little disorienting, and oddly embarrassing, to be on “the other side of the door.”
Anyway – Dr Vince Herr, the anesthesiologist, gave me some propofol so I don’t remember a thing; but when I woke up I was told that I had a small clot in my left atrial appendage, and turbulence in my left atrium as well. This was a surprise for everybody involved. Judging from my lab work and the bruises on my arms the Pradaxa seemed to be working – but evidently not well enough! And that “small clot” looked pretty big to me – downright dangerous.

Trail Running on the PCT
At that point I was immediately started on Lovenox injections twice daily (for six weeks!), the Pradaxa was discontinued, and I am beginning to take warfarin (Coumadin); and of course I stay on the beta blocker (carvedilol). My cardiologist gave me the first Lovenox injection right in the post-op area.
Also it looks like no running or bicycling for six weeks – which of course is devastating to me, emotionally, but – shit! – blood clot / stroke / potential death – yes, I am definitely sticking with the program!
The injections are easy to do, they burn a bit but don’t really hurt, and every injection leaves a bruise. Believe it or not I enjoy and look forward to each injection because I’m hopeful that they will be helpful.

I’m disappointed that the Pradaxa failed – it is much easier to take that warfarin. Remember that I am a vegetarian and one of my passions is eating healthy food, especially kale. Also everyday, up until now, I eat a little square of nori (seaweed – like the wrapper on sushi) thinking that it would be a good source of iodine as I don’t eat any seafood or use table salt. Kale and nori are probably the two worst foods to eat if you’re taking warfarin!
Taking warfarin is going to be a real challenge – changes will be made, changes that actually seem sort of unhealthy. The one advantage is that warfarin is, unlike Pradaxa, reversible, which is a true benefit in the case of a bike or auto crash, a GI bleed, a head injury, and so on.

Moore Park Trails
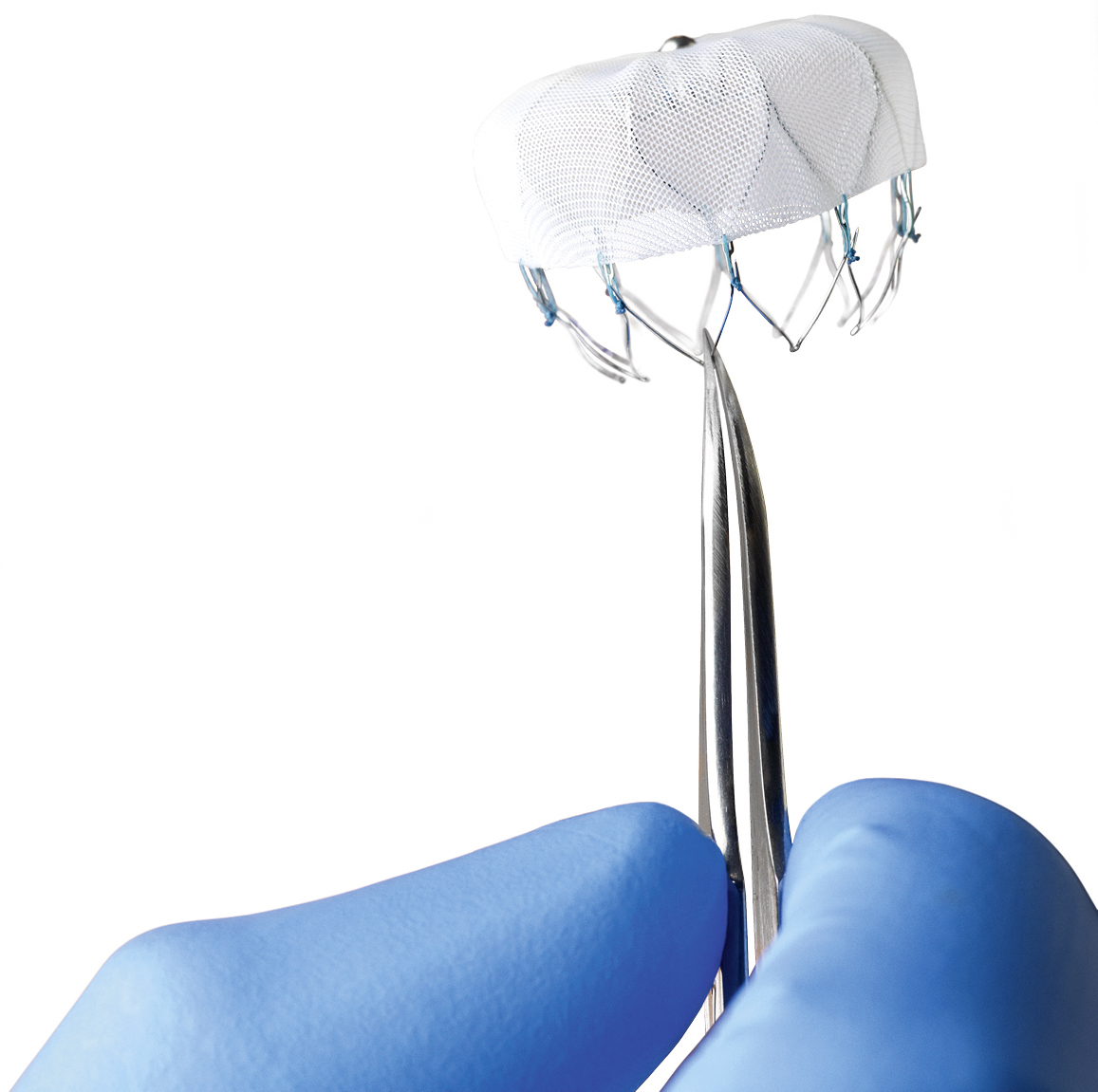
In six weeks the trans-esophageal echocardiogram will be repeated and hopefully the clot will be gone. If not some sort of procedure (by the electrophysiologist) is in store for me. Hopefully I will 1.) not die and 2.) get back to trail running. Until then my nerves are wracked worrying about having a major stroke!
I need to say that I feel incredibly blessed – if I hadn’t met my friends and stopped to chat I never would have known I was having a TIE. And if Linda hadn’t have texted me the next day I wouldn’t have ever pursued it, because I had, in my mind, completely dismissed it. And also – how many people actually have a neurologist right in their office who is willing to talk at any time?
Clearly I’m not through this yet – but in a way I feel I have already dodged a bullet. Really, if it weren’t for Linda that blood clot would have just kept getting bigger and who knows what would happen next? I might be dead by now. Even as it is now – who knows? But at least now I know I have a problem and the treatment plan has been changed.
So thanks, Linda!
Me and Linda in Costa Rica
I would appreciate any comments, especially shared experiences, you might have.
To be continued. Wish me luck.