I’m going to “ring my own bell” here and post that afibrunner.com has been chosen, once again, as one of Healthline’s The Best Atrial Fibrillation Blogs of the Year. Thanks so much, Healthline!
According to my WordPress dashboard I have a lot of views of my blog directed from healthline.com – I truly appreciate it.
It’s been a while since I have written and I have to say the last couple of months have been nerve-wracking. As I posted in a previous entry I had a TIA (transient ischemic attack) while running a couple of months ago, had a normal carotid scan, but a TEE (trans-esophageal echocardiogram) showed that I had a small blood clot in my left atrial appendage.
In other words I had a “mini-stroke” and was at risk of having a full on stroke.
This TIA occurred while I was on Pradaxa, a newer, novel anticoagulant. At that point I was taken off Pradaxa, started on Lovenox (low molecular weight heparin) injections, and warfarin (Coumadin), and also aspirin. I was instructed to discontinue running, and bicycling, and limit my activity to easy walks, and a repeat TEE was scheduled two months after the initial one.
I won’t hold back any longer regarding the surprise ending – I never had a second TIA “mini-stroke” (that I know of) or stroke and the follow-up TEE (trans-esophageal echocardiogram) showed that the blood clot inside my heart is now gone. Hooray!
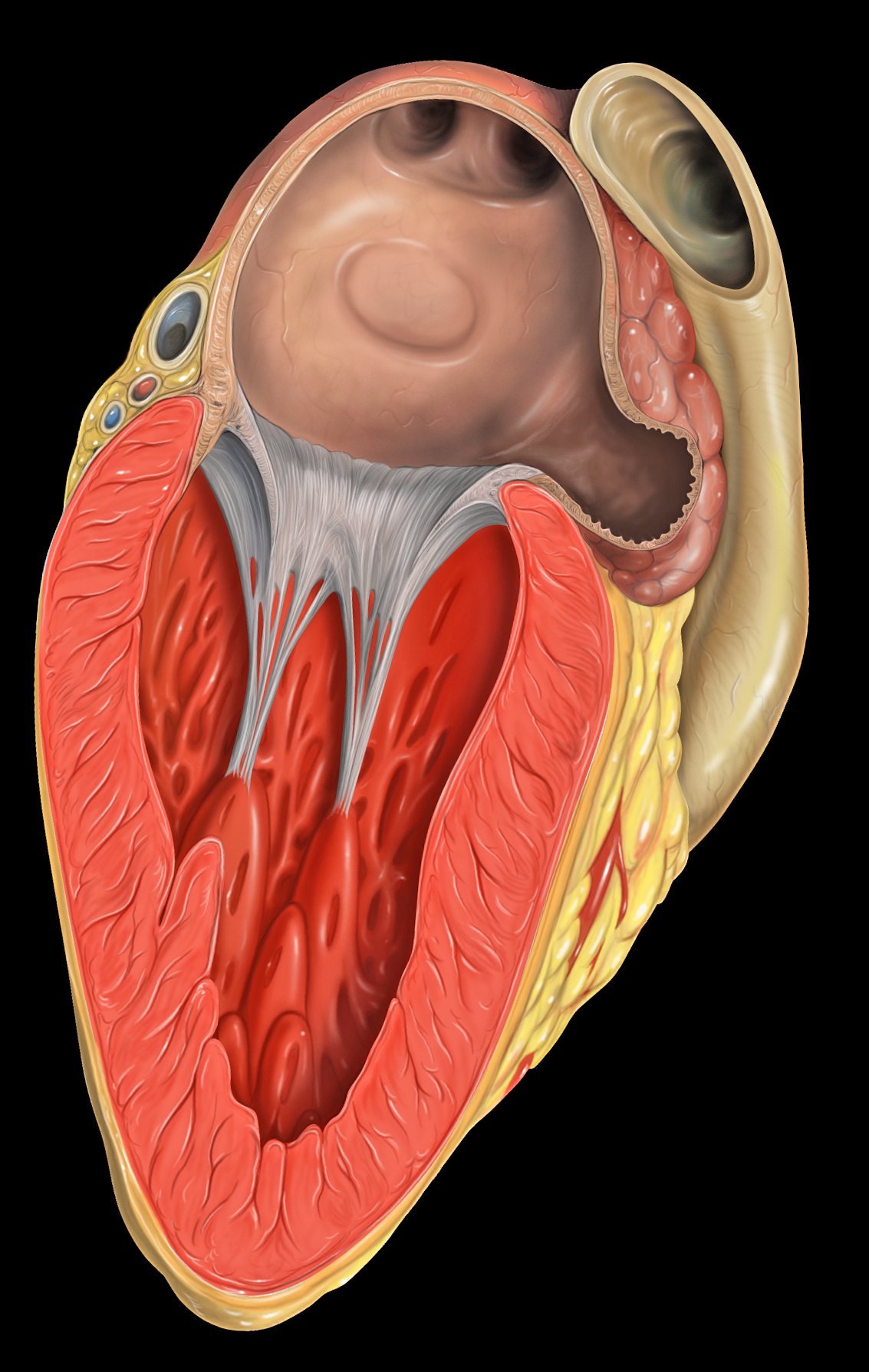
Photo – The little cul-de-sac is the LA appendage
Just to review how this happens: when you are in atrial fibrillation your atria is beating so fast it’s like it isn’t beating at all, just sort of vibrating. There is a part of the left atrium (the “appendage”) where the blow flow is extra sluggish, and this is where clots can form. When a tiny piece of clot breaks of and goes into the brain that’s a TIA. If a big clot is present and breaks of into the brain that’s a stroke, which of course can be disabling and even fatal.
It goes without saying that I am disappointed that this occurred while I was on Pradaxa. I figured that as long as I was taking it I was safe, and I liked not having to watch my diet or have blood tests constantly. Taking Pradaxa is easy – “set it and forget it.” Now I’m on warfarin (Coumadin), a royal pain in the butt, and have to micromanage my diet constantly – this drug is not an easy choice for a vegetarian! Eating too many greens (think kale) is dangerous as is not eating enough greens. Imagine trying to eat about the same amount of kale or broccoli or spinach each day.
Photo – vegan pizza
My target INR is between 2.0 and 3.0, but seeing as I have had a TIA while on an anticoagulant I am trying to keep it nearer to 3.0 or even higher (3.0 – 3.5).
The two months between echocardiograms was an era of angst – anxiety and fear – for me, especially the first several weeks. Every symptom, no matter how minor, seemed like stroke. For example – lie in bed trying to get to sleep and your hand becomes numb – normal, right? Not when you know you have a blood clot in your heart – that seems like a stroke! Jump up from bed, start testing the muscle strength in each arm and leg, recite the alphabet, smile, frown, move eyebrows up and down checking for asymmetry. Do you think I’m exaggerating?
Every once in a while a person stammers or mispronounces a word. Normal? Maybe, but not when you are obsessed with a gigantic blood clot lodging in your brain.
As far as exercise was concerned at first I was limiting myself to short, easy walks more appropriate for a non-athlete. Eventually I became a bit bolder and started doing longer (but slow, especially up hills) hikes of an hour or two. It took me three weeks (!) to bridge to a therapeutic INR, so I was on warfarin and Lovenox for all that time. Once I was off the injections I started doing bike rides – but they were on non-technical trails and were slow, especially while going uphill.
My brain never got the memo that I was no longer a long distance runner/cyclist so I still ate like I was, and consequently I’ve gained some weight.
At this point, after finding out the clot is no longer present, I have started increasing the intensity of my bike rides, but mostly I’m still doing bike rides. I haven’t yet started running again – but I will.
I am mountain biking again, but not on any trails that would be considered challenging. Well, that’s not 100% true, I guess.
Photo – “Adventure Without Limits?”
As far as mountain biking is concerned I am phasing out technical trails (gradually). I made a deal with my self that if I didn’t have the blood clot on the second TEE I would get a new bike – and I did. I got a Specialized AWOL, which is a “gravel grinder.” That’s sort of a cross between cyclocross bike and a loaded touring road bike – basically a bike designed for gravel or dirt roads – we have an infinite supply of these around here so I have a lot of exploring ahead of me.
As far as that blood clot is concerned I’m very pleased it has gone away – but I am not fooling myself that it is gone forever. It could return at any time. It wasn’t there when I had my second TEE, but it could actually be there right now – how would I know? How long had it been there and how many times have I had a clot in that area? There’s no telling without doing a ridiculously expensive, somewhat invasive test over and over. I guess all I can do is stay vigilant, take my meds, watch the diet, and keep on trying to run, hike, and ride, even if it is at a reduced level.
Some of the people who comment on this blog seem astounded that I can still run and bike while in atrial fibrillation. This surprises me because, at this point, I feel fine. Frankly just being on a relatively high dosage of a beta blocker (Carvedilol) is much more of a hindrance to my running than being in atrial fibrillation is.
But the big difference is that I am in permanent (constant) a fib. I’m used to it. And since I started taking the beta blocker I barely even notice the irregular beat. I’m slow now, and I get light-headed when I get up, but that’s it.
But recently I read a thread on a Facebook group, Atrial Fibrillation Information Exchange, and it was a real eye opener. I have forgotten how much other people suffer with atrial fibrillation. Here is a sample of comments (with spelling corrections) left in response to thread that asked:
Wondering what symptoms you get when in afib? What others feel and deal with?
-Rapid heart rate (220+), chest pressure/pain, dizzy, irregular heart beat, feel like I am going to lose consciousness.
-First my face feels warm,then the heart starts jumping erratically, can’t take an accurate pulse-then I know!
-I get a breathlessness, my rate stays low though but the overall feeling is like anxiety or the way one would feel before giving a speech or before competing in an athletic event etc.
-Mine is rapid heart rate,palpitations and anxiety
-All of the above plus hot and cold and violent vomiting. Also, if I’m sick, vomiting can bring it on
-Feels like there is a fish swimming in my chest, also weak and dizzy.
-Sweated and like your going to pass out , irregular and rapid heart beat , drinking cold water will help me convert, after I’m exhausted even will fall asleep haven’t had one in a few years now
-Like a squirrel doing back flips in my chest
-Felt like an anxiety attack plus tight feeling in throat( like it was dry and closing up) made me cough. Light headed/ dizzy, tired.
-I’ve had 8 AFib episodes since June of 2011. It always happens when I come out of a state of rest and stand up and start to walk. Except last month all I did was hiccup and cough at the same time and it triggered my AFib. Went to the ER and had cardioversion. I’ve never felt sick, dizzy, sweaty, breathless, nothing. Just racing heartbeat with strong palpitations.
-Mine was accidentally diagnosed initially on a routine office EKG.
-I get a “sinking” feeling in my chest.
-Flopping in my chest, weak, nausea, panic, sweaty, very very uncomfortable.
-I never come out of AFib. I had a stroke 5 years ago that affected my left side. I developed central pain syndrome in my left arm. So my heart sort of hurts and I have pain in my left arm.
-Weak breathless chest tight
-I had no symptoms other than lack of sleep and then the symptoms that go along with that. And symptoms from the meds. Oh, and the stroke.
-Sometimes it’s real quick flutters, or a skipped beat, I feel weak, sluggish, my chest hurts a little, and sometimes I get flushed and feel real anxious and nervous for awhile.
-Anxious & funny feeling in chest
-It’s almost like it’s gonna be an anxiety attack, but never goes to one thank goodness
-I have had episodes so bad I thought I would die. Then while in a fib, having to urinate every five minutes. It was like my body was in total rebellion. Sudden movements can trigger. Stress is a biggee.
I need to consider myself fortunate that I am so stable and feel so normal in permanent atrial fibrillation. I can recall what it was like when I was in sinus rhythm and would go into atrial fibrillation, usually during a long run, or even during a marathon – this is how I felt: I felt like crap – weak, mild malaise, light-headed, with vague chest and shoulder pain with exertion. Not pleasant by any means.
I’m curious – how do other fib runners feel while in atrial fibrillation? Please feel free to comment below.
About two weeks ago I was out for my typical Saturday two hour trail run on Moore Mountain with my dogs. It was a fine day and I felt great, and with about ten minutes left in the run I ran into three of my friends who were out mountain biking. My friend Linda, a Physician Assistant, was trying out her fancy new mountain bike and we stopped to talk for a while. She showed me her new bike and I introduced her to my new dog. I noticed, and commented, that I was having a little trouble getting my mouth working properly. I didn’t have any trouble finding words, or even saying the words, but my tongue just felt sort of thick – especially with consonants like “R” that seem to be made in the back of the mouth. I immediately did my self inventory for asymmetry and muscle weakness and found none. I attributed it to having had one of those little, annoying white sores in my mouth, accompanied by some swollen glands and thought nothing of it.
Linda Cyclecross racing
I finished my run, which involved a fairly technical descent, ate my post-run Clif Bar, and went home where I noticed nothing amiss. I forgot about it until Linda texted me the following day asking how I was doing and saying she was worried about me. I assured her – I was fine!
The next Monday, at work, I thought I’d ask my friend and co-worker, Dr Zakir Ali, if he thought the incident was any reason for concern. Dr Ali is a neurologist who works a couple of days a week at the orthopedic clinic, where I work as a podiatrist.
He wasn’t as dismissive as I was about the incident and said that that was very suspicious for a TIE (transient ischemic episode). A TIE is basically a small, brief stroke, in this case likely caused by a small blood clot that resolves fairly quickly. Dr Ali said I should, at the very least, get an echocardiogram to see if there is a clot in my left atrium, and possibly a carotid artery scan as well.
I have been in permanent atrial fibrillation and on Pradaxa, a potent anticoagulant (blood thinner) for two years and had never missed a dose. I thought he may have been over reacting – and I had had an echocardiogram just two months ago.
But Dr Ali had told me, “You will never regret checking.”
And I agreed.
Okay.
So I called the on call cardiologist, explained what had happened, and he told me a standard echocardiogram would be useless as it won’t show a clot, and recommended a trans-esophageal echocardiogram, and also a carotid scan (ultrasound).
I mentioned that I had had a trans-esophageal echocardiogram before (in 1994!) and it was like swallowing a telephone. He said he’d get anesthesia involved and we set up both procedures not expecting to find anything.
So the carotid scan came first and was normal, as expected.
Last Wednesday I went to the hospital and checked in to Day Surgery – which was a peculiar and strange experience for me. I’ve been working there, as a surgeon, for the past twenty-five years, but this was my first time being there as a patient. It’s a little disorienting, and oddly embarrassing, to be on “the other side of the door.”
Anyway – Dr Vince Herr, the anesthesiologist, gave me some propofol so I don’t remember a thing; but when I woke up I was told that I had a small clot in my left atrial appendage, and turbulence in my left atrium as well. This was a surprise for everybody involved. Judging from my lab work and the bruises on my arms the Pradaxa seemed to be working – but evidently not well enough! And that “small clot” looked pretty big to me – downright dangerous.
Trail Running on the PCT
At that point I was immediately started on Lovenox injections twice daily (for six weeks!), the Pradaxa was discontinued, and I am beginning to take warfarin (Coumadin); and of course I stay on the beta blocker (carvedilol). My cardiologist gave me the first Lovenox injection right in the post-op area.
Also it looks like no running or bicycling for six weeks – which of course is devastating to me, emotionally, but – shit! – blood clot / stroke / potential death – yes, I am definitely sticking with the program!
The injections are easy to do, they burn a bit but don’t really hurt, and every injection leaves a bruise. Believe it or not I enjoy and look forward to each injection because I’m hopeful that they will be helpful.
I’m disappointed that the Pradaxa failed – it is much easier to take that warfarin. Remember that I am a vegetarian and one of my passions is eating healthy food, especially kale. Also everyday, up until now, I eat a little square of nori (seaweed – like the wrapper on sushi) thinking that it would be a good source of iodine as I don’t eat any seafood or use table salt. Kale and nori are probably the two worst foods to eat if you’re taking warfarin!
Taking warfarin is going to be a real challenge – changes will be made, changes that actually seem sort of unhealthy. The one advantage is that warfarin is, unlike Pradaxa, reversible, which is a true benefit in the case of a bike or auto crash, a GI bleed, a head injury, and so on.
Moore Park Trails
In six weeks the trans-esophageal echocardiogram will be repeated and hopefully the clot will be gone. If not some sort of procedure (by the electrophysiologist) is in store for me. Hopefully I will 1.) not die and 2.) get back to trail running. Until then my nerves are wracked worrying about having a major stroke!
I need to say that I feel incredibly blessed – if I hadn’t met my friends and stopped to chat I never would have known I was having a TIE. And if Linda hadn’t have texted me the next day I wouldn’t have ever pursued it, because I had, in my mind, completely dismissed it. And also – how many people actually have a neurologist right in their office who is willing to talk at any time?
Clearly I’m not through this yet – but in a way I feel I have already dodged a bullet. Really, if it weren’t for Linda that blood clot would have just kept getting bigger and who knows what would happen next? I might be dead by now. Even as it is now – who knows? But at least now I know I have a problem and the treatment plan has been changed.
So thanks, Linda!
Me and Linda in Costa Rica
I would appreciate any comments, especially shared experiences, you might have.
The last article I wrote about beta blockers was written last Summer when I was more or less just starting the beta blocker. I had noticed a decrease in performance and exercise tolerance and when I went to the cardiologist and had an echocardiogram it was determined that my rate was going up and my ejection fraction was going down – that means my heart was pumping less efficiently and was pushing out as much blood with each beat. I was put on a low dose of carvedilol (6.25 mg twice daily) and it was thought that this would allow my ejection fraction (EF) to come back up.
When I started my EF was 55%, but when I had the echocardiogram mentioned above it was down to 45%. As noted in my last beta blocker article I suffered on runs and bike rides but felt it was worth it as I anticipated improvement.
When I returned for the follow-up echocardiogram I was extremely disappointed to learn that my EF had actually gone down to 37%. Not good.
At that point I the dosage of my beta blocker (carvedilol) was titrated up from the minimum dosage to the maximum dosage (50mg twice daily).
As you might imagine between the atrial fibrillation, the decrease in EF, and the high dose of beta blocker – running became extremely difficult. All three of these things decrease my cardiac output and, of course, that translates to poor performance. I now found I had slowed to a ludicrous pace, and honestly, running was starting to become a chore.
Running was starting to become unenjoyable; but I continued anyway.
I felt like every run was my first run after not exercising for several years, and I was walking up the most minor hills.
Last week I returned to the Heart Clinic and had yet another echocardiogram. To be honest I haven’t been feeling any better and runs still seem difficult so I decided not to even look at the screen or ask the tech about my EF as I assumed it was still poor. I’d just wait until the follow-up appointment with the cardiologist. But the tech, who knows me by now, just came out and told me – “Well, it looks like your ejection fraction is improving – it’s up to 47%.”
Well, that is good news. At least this suffering through the beta blockers is leading to some benefit.
That was just the preliminary reading, my new cardiologist (my previous cardiologist retired from clinic but still works at our hospital) interpreted the echo and said it was more like 50%!!! That’s nearly back to normal range (52-70%).
One interesting thing the cardiologist told me: she said that one would expect that people who are more athletic would have higher ejection fractions than non-athletes but in reality the opposite is often the case. I told her that my heart is so big that if my ejection fraction was too high there would be too much blood – ha ha.
There’s something I don’t understand about echocardiograms and atrial fibrillation – as anybody who is in a fib knows some beats are better than others. It’s easy to feel that – some are short and weak and others are longer and more powerful. How, when looking at the heart with the echo machine, can you tell what kind of beat you are having?
So there is some good news. Runs are still difficult and I don’t see myself ever being completely off of the beta blocker – but hopefully a different dose in the future when my ejection fraction reaches whatever the goal value ends up being.
In my next article on running and beta blockers I will discuss “Beta Blocker Blues” and the way this unpleasant medication makes me feel fatigued and, often, quite depressed. But for now I’ll embrace the joy of knowing my ejection fraction is significantly improving and will likely get even better.
I have been in permanent atrial fibrillation for a couple of years now, but only been taking an anticoagulant (Pradaxa). But things have changed and for the past month I have been on a beta blocker, carvedilol.
Prior to starting the carvedilol, while in permanent atrial fibrillation, I had been able to run two marathons and one ultramarathon (50K) without any more trouble than the normal marathon type suffering, but over the past six months I have noticed things have been changing. I’ve slowed down, even for me, and distances are getting harder. My last half marathon was a joke and I was at the end of the pack within the first two miles. After a run or mountain bike ride of an hour or more I would have problems afterwards – my blood pressure would drop and my pulse would stay high. After a long run, especially if it was a hot day (which they all are, recently) I would get so light-headed after standing up I sometimes had to grip onto something to remain standing.
A visit to the cardiologist, and a subsequent echocardiogram, revealed that my heart rate was increasing and my ejection fraction was decreasing, and for that reason the cardiologist wanted me to start on a beta blocker.
A beta blocker, in this case carvedilol, is a drug that reduces stress on the heart by slowing the heart rate, decreasing the force with which the heart beats, and reduces the tone of the arteries throughout the body. The end result is that blood pressure is reduced, as is heart rate. The heart needn’t work so hard.
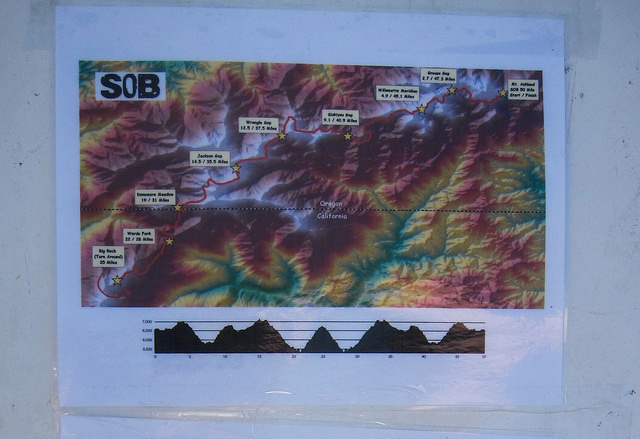
SOB 50 Mile Course – tough!
Some non-endurance athletes actually use beta blockers as performance enhancing drugs – it is said that it calms a person, reduces performance anxiety, and is commonly used in less endurance specific sports such as golf, target shooting, archery, and even in music performance.
Clearly these drugs are performance diminishing for endurance sports like distance running and mountain biking. We like to stress the heart, raise the heart rate, and we don’t have very much stress – we’re long distance runners after all – the mellowest people around.
I generally am in at least half marathon shape year round. Even if I’m not training for anything my weekend long run is going to be between nine and twelve trail miles. Prior to starting the beta blocker I had signed up for the 15K at the SOB Trail Run at Mount Ashland (Oregon) – one of my favorite races. This relatively high altitude run is basically all up and down trails and fire roads (zero flat sections) and I have done it at least six times in the past, including completing it twice in atrial fibrillation. I was curious to see how being on the beta blocker would affect my race.
DNF
The answer was I DNFed (did not finish) and dropped out fairly early in the race. That was terrible – most of my friends were running the 50K or the 50 mile and I DNFed the little 15K???
The course at the SOB is brilliant, really. A lot of trail races start out right away on singletrack, but the SOB has about a mile(?) of fire road at the start so everybody has plenty of time to figure out whether they are going to be running with the fast people or the slow people before they hit narrow Pacific Crest Trail. I ended up at the very back of the group that was running, but I was still in front of the few people who were walking the 15K.
I found that as soon as the course headed up hill I was unable to run. My chest felt funny – not chest pain, just felt weak, not right, and my legs felt dead. I wasn’t short of breath, I was just unable to do it. I decided, in my typical OCD mode, to continue running for five more songs on my iPod shuffle, and then turn around and drop out, thinking that I should at least get a little bit of a work out in, and that I could justify keeping the T-shirt I had paid extra for. I knew I could have walked the course, but that is not what I went there to do.
I was delighted that the fifth song on my iPod turned out to be an oldie from my high school days: Yours is No Disgrace by Yes. Not actually I song I still like very much, but in this context it seemed like a cosmic pat on the back.
On the way back I met a woman who was also DNFing (sprained ankle) and we walked the last section of the race together, commiserated, and removed our numbers so they wouldn’t mistake us for the top finishers. At the finish line we informed the race officials that we had dropped out so they didn’t need to send a search and rescue team to find us.
DNFing and commiserating together as we remove our race numbers
So this article is, basically, my first impression of being on a beta blocker, in addition to the atrial fibrillation, and trying to remain an endurance athlete.
So far I feel that the beta blocker is more of a hindrance to my running and cycling than the atrial fibrillation alone had been – but then again, because of the atrial fibrillation my heart function is gradually diminishing.
I should say, on a positive note, that the beta blocker is working, and is doing what it is supposed to do. I check my heart rate and blood pressure at least once per day and since I started the carvedilol I am right where the cardiologist wants me to be. And I can understand why people who aren’t trying to be athletes might like the med – it seems to have a mild calming effect. Furthermore I no longer feel like my heart is a fish flopping around in my chest, and my post work out blood pressure and heart rate has stabilized.
I am optimistic that the carvedilol will be worthwhile and will help me preserve and regain my ejection fraction. But really, what choice do I have?
So here is how things have changed so far (compared to just permanent a fib without the beta blocker):
1.) As far as mountain and road biking is concerned I have been able to ride all the hills that I used to be able to ride, although I am much slower. My wife now has to wait for me at the top of a climb, and that’s fine. I am delighted I can still ride and don’t have to get off and walk my bike.
2.) Running is more negatively influenced. My previous slow pace is even worse, and hills are quite difficult. Not surprisingly I do not like this one bit. A slow jog feels like a 5K effort. But I am still able to run – Yay!
3.) Long runs in heat are not possible. I am just not able to do a long run in heat, and lately every day has been warm. Understand that I am a big red-faced Irish-American who considers anything over sixty degrees to be hot running weather; plus I live in a very sunny place, a high desert climate without a lot of shade. It is not surprising that this is happening. A normal person running in heat will have a higher heart rate for a given pace, and will need to slow down. If you are on a beta blocker that reduces the maximum heart rate by a significant amount, well: “game over.”
My goal is to continue running and mountain biking on trails like this: Brown Mountain Trail
4.) I suspect that the beta blocker might be making me lazy. I don’t know if that is the right word, but I had a full day off in the middle of the week a while ago and I had planned on, among other things, writing this article and going for a trail run, and next thing I knew it was late afternoon and I hadn’t done a thing. What? By that time there was a thunderstorm so I was not going out for a run – but the article still hadn’t been started. I hope this is not going to be the case from now on. Being lazy and depressed is far from my idea of fun.
I am going to wait until I have had more experience with the beta blocker and write a better informed article. I’m going to sign up for a relatively flat (downhill, actually) trail half marathon and try to redeem myself.
In the meantime I would love hear about other people’s experiences with the dreaded beta blockers. Please post a comment below.
This is Joe’s Story – a guest blog article based on Joe’s comment on this blog describing his fascinating experience with atrial fibrillation and subsequent heart failure. Joe has really demonstrated persistence and a positive attitude that, I think, a lot of athlete’s with atrial fibrillation possess. Joe is making a comeback from serious, life-threatening heart failure, and he has done a good job of accepting the new reality of his post a fib performance.
+++++++++++++++++++++++++++++++++++++++++++++
Joe Triumphant
Hi Everyone – I’ve had A-Fib for about three years now.
I live in the tropics and cycle, run, do weights. I train five days a week but not hard or too easy. I believe I got into this mess when I cycled up our small mountain here on the island I live on three times a week back then. I would only drink reverse osmosis cleaned water consuming about four liters just going up the mountain. I’d do weights in the morning and cycle in the afternoon and believe me it gets hot and humid. It’d take me about two hours to cycle up to the top of this very very steep course. (approximately 5K to the top)
In hindsight now I guess I’d been over-training terribly and not putting back potassium and minerals into my body at all. I happened by luck (or fate) to be given a heart monitor and thought it was cool to use it on my cycle ride up the mountain. I set the max at 185 and started off – as soon as I started up the steep hill after a five kilometer preamble the damn thing started beeping – it was at 205 and I just started up the hill! Like an idiot (ha ha) I kept going and it would not shut up. Did it the whole way up and for the next month it was like that. Can’t believe it now I did that but as I’m in constant A-Fib now the reality speaks for itself.
Been put on beta blockers and have to take warfarin. I suffered a sever influenza sickness last year and it really took a toll on my ticker. My left ventricular ejection fraction (LVEF) was only 17% when I finally went to see the Cardiologist here as the echo showed.
Fast forward now to a month and a half and I’m back up to 35%. The goal is to get back to 55%! I love running and exercise and like some of you wrote would rather plonk on the trail then sit on the couch, so be it. I used to run with the goal of just finishing the run and was happy about it.
This is Joe’s heart on heart failure
Then I got into times, was happy about that too. Before my illness last winter my times were at my all time best. Slow for a lot of runners but for me great. After all I run to please me so I accept what ever pace I come home at. Not a biggie. The doc was amazed at how fast my heart recovered and I even saw the difference on the screen of my heart’s movement. The echo I had before it looked like Jabba the Hutt sleeping. I think I attribute this to doing a LOT of research on the internet getting informed of what I was dealing with and trying it slowly with my Doctor always in the know. He was very skeptical of the supplements I was taking but has done an about face now. I also believe the coconut water I drink everyday now has helped in a big way. I noticed I don’t have an ammonia smell anymore when I sweat. I always had that smell when I drank the Osmosis water. I drink a mineral water now along with the Coconut water.
Anyways – I do prattle on. The thing is not to Panic and get informed!
I wear a Polar T-80 watch with GPS and follow the Zone rules. Yeah, I’m running about four minutes slower than normal but I feel great after a run now and do not dread the next one. Hoping my pace will kick up a notch as the info says it will as the body adapts.
This forum is great may I add and it sure is reassuring to read of Peep’s in their 80′s who’s lived with A-Fib for 20 or so years and keep running. Hopefully one day soon someone will find a cure for this curiously annoying ailment.
When I had 17% ejection rate it happened really fast. The time line is like this: on a Friday I ran a very fast 5K run for me. One of my best times. Later that day flew to spend three days with a friend, and after returning home I got ill and by Wednesday was full blown into whatever ailment I had (Influenza?). I tried running a week later but could not even go further than 50 yards! Then I stopped and decided to rest a week, do nothing and fight this illness. Well, it got worse and worse – my lungs started filling up with fluid and at night I could hear bubbling in my lungs. Fast forward a week of no sleep, etc, etc, and went to a doctor was put on antibiotics. I didn’t get better, still the same symptoms. (Turns out the heart, because of it not beating properly causes the fluid to back up and then it seeps into the lungs so any of you with these symptoms see a doc. You can do a thumb press on your shin and if the indentation stays and is deep you’ve got fluid retention and need a diuretic).
After a couple more weeks of this I decided because of previous symptoms I felt there was something wrong with my heart again. Seemed to be doing the same old symptoms of A-Fib. I thought I was free of it for almost two years or else it was Silent A-Fib and I did not know it!
My cardiologist gave me an echo and all he said was “What did you do?” Man, you don’t want to hear that from your doctor!
Like I said before I even could see my heart wasn’t doing anything. Just sort of sitting there: legs up – arms crossed!
He put me on meds again and the dreaded warfarin. They worked almost right away! I was on Codarone (amiodarone) for only a month and everyone should know that this is a dangerous drug! Long half life and it’s like shaking hands with the devil. Used a lot as a last resort. But! – for short periods it works miracles. Using it over six months or more can have repercussions.
Well, that day I came home from the doc’s I tuned up my mountain bike and went for a very short ride. I was out of breath the whole time. Did this for a couple of weeks and got stronger. Started weights again, and just started using the bars with no weights. Did this very very slowly and now after two months I’m almost back to benching 200. (ha ha – good for me anyways) The last check up the doc said my heart (Left ventricular ejection fraction) was up to 35% and I saw the difference in the video as well! Made me feel very very happy.
So now I’m trying something I never thought I’d do. I bought a Polar T-80 Heart monitor with GPS and run and cycle in the Zone. I exercise according to my heart rate. I’m finding I’m no longer exhausted during the rest of the day and overall feel better, stronger. It’s taking time to lose that competitive spirit though – ha ha ha – I’ve got friends who are in their 70′s running faster than me. My slowest times in years but I’ll stick to it and see if my times automatically come back up as the research suggests. This has to be done. I love being active but I hate being dead more so I have to accept and live accordingly. Don’t Panic!
A heart pumping at 33% efficiency feels a lot better than 17% I can tell you. I do more things than most of my friends. It still amazed me though how I can do weights for a hour, run for an hour then eat, chill and later in the day walking up a flight of stairs takes my breath away. It’s like a reminder – oh yeah I’ve got heart problems. A friend wisely told me that it could be like losing weight: fast in the beginning; then slower. I hope my ejection fraction % will keep increasing till 55%. Considered normal. Then I’ve got to deal with the A-Fib.
Joe still the life of the party – but no more beer for this guy!
A very important footnote: I used to drink beer everyday for years! Love the amber fluid. After my first A-Fib about five years ago I stopped for about three months. Then about two years ago I only drank on Friday and Saturday. For two years I did this. No exceptions. I’m 51 now and even this was taking it’s toll I believe. Now I’ve cut it out completely and will go the distance – sort of sucks but I’m close to the three month period now and will keep going. My next visit to the docs is in August so I’ll hopefully remember to post what transpires.
If anyone is interested in what I’ve been taking for supplements, eating, drinking, and exercising please leave a message on this blog and I’ll be most happy to share. One thing I’ve always found frustrating with most blogs is when I’ve read what someone has done and it worked there was no follow up. I’ll try and keep posting on this one. Great site! Peace out…………… don’t Panic : )
+++++++++++++++++++++++++++++++++
Update (from Joe)
Hi everyone. Went for my one month checkup at the cardiologist today and the results were better and improving. The Doctor said my heart has shrunk by a noticeable margin which is a good sign. (had an echo) It’s getting stronger. The ejection fraction went up a bit as well to around 37%. Getting nearer to 40% then in a few months hopefully 50 or 55%!! I was also able to wean off one med by half. I felt it in my run today – a really great run. Will continue on meds and supplements plus exercise and diet as is for another month. See ya then!
Is distance running therapeutic? Is mountain biking addictive? Is there such thing as a good addiction? If my atrial fibrillation worsens and I could no longer do long runs or bike rides – how hard would it be to kick the habit?
High Lakes Trail – Southern Oregon
Today in the hospital lounge, while I was eating some potato chips, somebody was telling me how bad potato chips are for me. Whatever – I have given up almost everything in the world that is bad for me. I haven’t drank alcohol in several years, haven’t smoked a cigarette in decades, gave up meat and eggs a couple of years ago, I’m almost dairy free, and I haven’t taken recreational drugs since high school in the seventies. Potato chips, which I feel are good enough to be “worth it,” are about it for me. Well, that and diet soda, which is also an unhealthy habit that I have.
But what about “runner’s high?” Is that my addiction?
And what exactly is runner’s high? Does it even exist? I’ve been hearing about it for a long time, even before I started running in the early 80s.
Allegedly the athlete’s brain is “flooded with endorphins, more powerful than any street drugs!”
Many distance runners claim to experience euphoria during or after running, and some claim they’ve never had it happen – not even once.
The endorphin theory is the oldest, but more recently I’ve read about how endocannabinoids (naturally occurring neurochemicals related, in a way, to the active ingredient in cannabis) might be the cause of runner’s high.
Whatever the cause, it certainly appears to be real.
Pacific Crest Trail via Brown Mountain Trail – Klamath County, Oregon
Ultrarunner Dean Karnazes describes the role that running has in his life: “Some seek the comfort of their therapist’s office, other head to the corner pub and dive into a pint, but I chose running as my therapy”
“I’m convinced that a lot of people run ultramarathons for the same reason they take mood-altering drugs. I don’t mean to minimize the gifts of friendship, achievement, and closeness to nature that I’ve received in my running carer. But the longer and farther I ran, the more I realized that what I was often chasing was a state of mind – a place where worries that seemed monumental melted away, where the beauty and timelessness of the universe, of the present moment, came into sharp focus.”
― Scott Jurek, Eat and Run: My Unlikely Journey to Ultramarathon Greatness
Actually, a recent New York Times article states that on good experimental evidence it has been finally determined that exercise does indeed produce a flood of endorphins in the brain. Lucky us!
Researchers in Germany, using advances in neuroscience, report in the current issue of the journal Cerebral Cortex that the folk belief is true: Running does elicit a flood of endorphins in the brain. The endorphins are associated with mood changes, and the more endorphins a runner’s body pumps out, the greater the effect.
I won’t review the article here, but please read it – an elegant experiment, and solid conclusions.
But irrespective of the cause, what is runner’s high and what does it mean to endurance athletes? Can a person become addicted to it?
Personally I feel that the term runner’s “high” is a misnomer. I would describe it better as an altered state of consciousness rather than a high. Maybe I’m splitting hairs but I have never felt intoxicated by endurance sports.
Euphoria might even be too strong of a term – but maybe not. There are times during and after running when everything appears exceptionally crisp and beautiful. That’s why I love trail running, in Oregon, in the wilderness – does that happen to people in health clubs running on treadmills?
After an hour or so even carb gels seem remarkably delicious!
Also – music becomes intensely enjoyable. I do run with an iPod and sometimes I feel I am going back to the days back in high school when I smoked pot and would listen, chemically enhanced, to suddenly amazing music on headphones. Except now instead of sitting in a darkened basement I’m moving through the woods. It’s funny – a lot of the music that, for me, is most enjoyable on long runs, is the same type of music that I believe would be most enjoyable to a person who is stoned. Sometimes a song sounds so good I’ll repeat play a song two or three times.
But another reason I don’t like the title “runner’s high” is it isn’t all euphoria, beauty, and music joy. I think the exercise induced altered state of consciousness can involve a certain amount of emotional lability. Here’s an example: once I was on a twenty mile trail run, and at mile sixteen an old song I hadn’t heard in years, Careful With That Axe, Eugene, started playing in my random shuffle. This very early, nine minute long Pink Floyd song is sort of a novelty song; a one chord song that slowly builds on a rising and falling bass line with a mellow organ playing over it. At one point a whispering voice says, “Careful with that axe, Eu-zhene.” And then there is this horrific screaming and dissonant guitar, and finally it evolves back to the mellow bass and organ. Back when I was in high school, if we had somebody over who had never heard the song before, we’d put it on and turn down the lights, and of course when the screaming began it would scare the crap out of the first time listener, and we’d all have a good laugh.
Well I knew all about what was going to happen during that song and wondered if I would start laughing when the “axe” section came up. Imagine my surprise when I burst into blubbering tears when the screaming began. I should state that this was shortly after my ex-wife (with whom I was still friendly) and her family had died in a horrible house fire – but honestly I wasn’t even thinking about that until the screaming in the song. I know I wouldn’t have been anywhere near that emotional if I hadn’t just put in sixteen hilly trail miles.
Other times while running something will strike me as funny I will begin laughing giddily – out there all by myself, or in the back of the pack at a marathon. Or an angry song will play and I’ll feel, like, GRRRRRRR!, become angry – quite a catharsis.
GRRRRRRRR!
So is exercise induced altered state of consciousness addictive? I’m thinking: yes.
C – Have you ever felt you needed to cut down on your running? A – Has anybody ever annoyed you or criticized your running? G – Have you ever felt guilty about your running? E – Have you ever felt you needed a run first thing in the morning (Eye-opener) to steady your nerves?
Well – I can honestly say I’ve never felt guilty about my running, but the rest of those questions, well . . . .
And I can state for the record that with my atrial fibrillation, and the likely progression of my a fib, including my upcoming need to be on a beta-blocker, I have been dreading the day when I am no longer able to run. Very depressing.
Biking in A Fib – like riding through mud
Aside from that I have a theory. I think it is obvious that not everybody will experience anything like a runner’s high. Clearly many people hate the way running makes them feel, and they are the people who think distance runners are completely nuts. And why wouldn’t they? Based on the time they ran two miles and felt nothing but fatigue and pain, and interpolating that up to, say, thirty-one miles, their obvious conclusion would be “WTF?” to use the parlance of our times.
Lyon’s Trail – Lava Beds National Monument
But as for myself, and I’m guessing most of the people who would be interested in this blog, the so-called runners high can be generally considered to be a gift.
Diversion: How to talk to your children about distance running:
This article is a work in progress and is only a description of my strategy for the time being. I hope to learn from readers of this blog about how to better plan for a trail debacle.
Heading out for a trail run on the Pacific Crest Trail
What kinds of things should a person like me, who is dealing with atrial fibrillation and is taking an anticoagulant (I take Pradaxa), carry on a long run in the wilderness? Or during a long mountain bike ride in remote areas?
When the high country in our local wildernesses is not covered with snow, I will generally do runs, nearly every weekend, of anywhere between six to twenty miles. I almost always run alone (except for my trail buddy – Ringo).
Dangerous and a bad idea? Possibly. But this is what I enjoy in life so I don’t plan on stopping any time soon.
The most important piece of equipment is a phone. People complain that everybody is always on their smartphone, and they should NOT be talking on their phones on mountain summits when everybody else is trying to get all Zen-like and self-actualized, and whatever – that’s a different discussion. You certainly don’t even need to have your phone on; but you absolutely should take it with you, and it should be fully charged. The days of getting hopelessly lost and spelling out SOS with rocks hoping a search plane will find you are fading into the past. A smartphone is a GPS and a direct link to help.
I always carry my iPhone in a baggie with my ID and a sheet of paper towel (which I use for unrelated toilet purposes).
Fully charged and protected from water
Even if there is poor cell phone coverage in your local high mountain or deep canyon wilderness, and a phone call isn’t always possible, I find that a text message can often still be sent. It might take a while but it eventually will be sent, especially if I am moving along a trail.
There is the standard emergency gear that most people take, often called the “ten essentials” which most people carry while in the wilderness. Of course there is truly no such thing as a standard ten essentials and the list of things you carry will vary depending on the season, your skill set, your location, and your past experience.
My generic survival gear
I got out my little survival kit that I typically carry in the wilderness, and of course not everything is pictured here, and I might not even have all of this stuff with me on any given trip. Naturally I will also have other things like food, gels, electrolytes, a jacket, and plenty of water.
What I found in my default wilderness pack is:
Two knives – a mini-leatherman tool and a standard knife. I will only actually carry one of these.
Two lights – a headlamp and a tiny LED flashlight (one is plenty).
Fire starter – a cigarette lighter, birthday candles, a tampon, and hand sanitizer (which I discovered has completely evaporated).
Pain pills: Vicoprofen samples – okay they expired in 2000 but I’m guessing they are still good (at least for a placebo effect). Missing: Benadryl for allergies or yellow jacket stings, and I probably should have some of my Pradaxa in case I end up unexpectedly staying out overnight. Also missing: small roll of duct tape, safety pins, and my whistle!
Saint Christopher Medal
Oh, and there is a Saint Christopher medal. This one belonged to my grandfather. Well it probably won’t change anything, but it certainly couldn’t hurt. Feel free to substitute your own personal good luck charm.
But what about specific items for the runner on an anticoagulant? Is there anything else beyond the “ten essentials”?
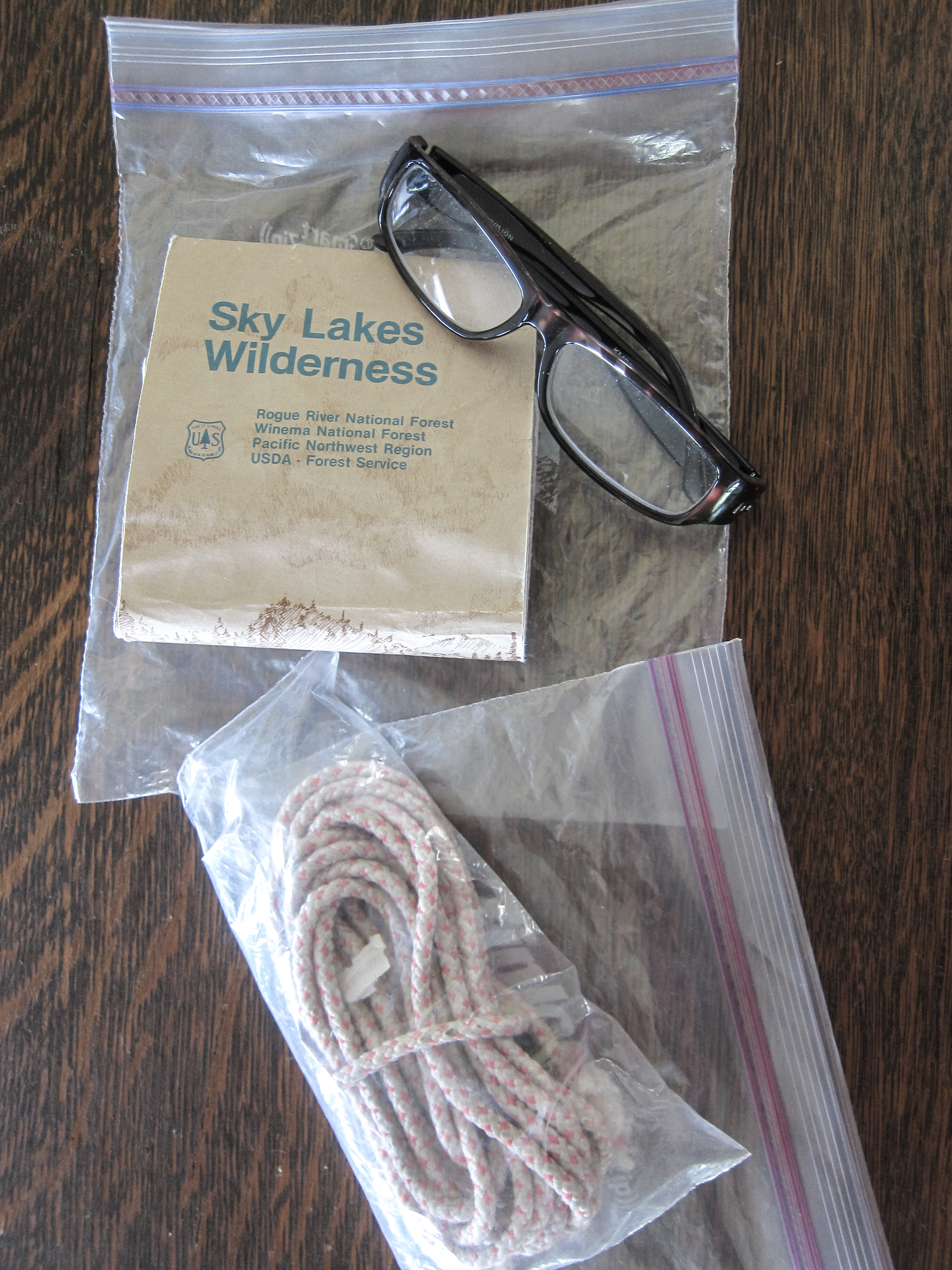
Other stuff: Map with reading glasses (if needed) and some rope
Obviously having a major bleed while running alone in the wilderness would be a disaster. Death is certainly a possibility. How can a trail runner prepare to increase the odds of a good outcome?
I always make sure to let somebody know (usually my wife) where I’m going and I also send her a text (I text “OOTW” short for “out of the woods”) when I get back to my vehicle.
I also wear a Road ID. This way if somebody finds me they will know I am on an anticoagulant. Maybe this won’t help, but it certainly is worth wearing. At least they will be able to figure out why I bled out so quickly (I know – not funny).
My Road ID
Another item I always carry is a bandanna. This can be used for a number of purposes, such as making a field dressing; but I want to have it in case I need a tourniquet. Plus – I have an extra one because my trail dog always has one draped around his neck.
Bandanna
My bandanna came in handy a week ago when my wife Margo (not on an anticoagulant) crashed her mountain bike and punctured her left thigh with her brake lever. I used it to make a compressive dressing before we road our bikes back to where we could get a ride to the hospital.
One item I do not currently have but definitely need to obtain is a Quickclot field dressing. Evidently these things really work and are routinely used in combat situations. It is a topical coagulant (an anti-anti-coagulant?) which helps clot blood and also serves as a physical barrier to bleeding. I’ve been meaning to obtain one of these for a long time. They are available online via amazon.com, and I just ordered one.
Quickclot
Question: Will the Quickclot sponge even work on bleeding in an individual who is on a direct thrombin inhibitor like Pradaxa? Answer: I have no idea. I’ll let you know if I ever get a chance to find out.
In case of bleeding the most important first step is to apply direct pressure. As a surgeon I have a lot of experience with this. Usually sixty seconds of direct thumb pressure will stop or slow most bleeding, but of course if you take an anticoagulant it will take longer. Apply direct pressure as long as necessary. Elevate the wound if possible. Don’t try to clean out major wounds as this will restart bleeding – that can be done later at the hospital.
A tourniquet is a last resort, but the bandanna can be used as a compressive dressing if needed.
Please understand that an anticoagulant doesn’t completely stop clotting of blood, it just makes it take longer. Eventually bleeding will stop. Hopefully before all the blood leaves your body!
Ringo always has a spare bandanna for me
Bonus – How to stop a nosebleed:
I have been plagued by frequent nosebleeds since I was a child but, oddly enough, I haven’t had a single nosebleed since I started Pradaxa a couple of years ago. The best method I have found is to pinch the nose, fairly tightly, just above the nostrils, and lean forward. Don’t lie with your head back – that doesn’t work. Hold for a full sixty seconds. Repeat as necessary.
If you are, like me, a trail runner or mountain biker on an anticoagulant, I would love to hear from you. Please leave comments and suggestions in the comments area below.
Hyponatremia (low sodium, or “water intoxication”) is a risk for runners with atrial fibrillation. It is certainly a risk for me and I believe I have experienced it a number of times in the past. Personally, I am much bigger than most marathoners (6’3” 205 lbs), and because of that and the atrial fibrillation, much slower – so I’m out there twice as long and sweating twice as much. Plus – over the years it has been drilled into all of us to make sure we drink enough water.
Ironman athletes, ultrarunners, and bigger runners are all at increased risk because we are simply out there for much longer periods of time. Women athletes tend to be at higher risk for hyponatremia – it has been found that women hydrate more during a race.
Drinking enough water is a good idea – but it needs to be accompanied by increasing salt intake.
Normal levels of sodium are about 135-145 mEq/L. Symptoms are likely to begin at 130 or lower and if you get below 120 the condition may become fatal. While there are a number of medical causes for hyponatremia marathon runners fall into the category of consuming too much water and not enough sodium, and sweating out valuable sodium. Think of the white dried salt on your temple or on your hydration pack straps after a long run.
Symptoms include bloating, headache, swelling (check to see if your ring or wristwatch seems to be getting tight), nausea, vomiting and eventually weakness, restlessness, confusion, and well . . . it just gets worse from there. It is particularly problematic for runners because some of the symptoms (headache, nausea, cramps, and dizziness) are the same symptoms for dehydration so the impulse is to drink more water – which of course makes it worse.
There is currently an ongoing study at the Houston Marathon involving volunteers who are followed closely, weighed, fluid intake measured, lab studies obtained, etc. The study found that runners with lowered sodium levels drank more water, retained more water than normal volunteers, and they lost more total sodium and had saltier sweat.
Runners who were dehydrated but not hyponatremic had higher heart and respiratory rates, felt worse, and had lower blood pressure than hyponatremic runners. The hyponatremic runners felt better, but had more nausea and bloating.
What can be done?
Drinking less water is sometimes recommended but it is difficult to do when you are used to drinking a lot of water while running. I’ve tried drinking less water during a marathon and frankly I think it made things worse. Also some runners can become hyponatremic without over-doing the water consumption.
Weighing yourself frequently along the course and looking for weight gain (water retention) has been recommended – YEAH RIGHT! How is this going to happen?
Personally I try to drink water with sodium supplemented (NUUN, GU Brew), and try grabbing some little pretzels at aid stations (if available); but some research suggests this might not always be helpful.
Fatigue? Really? Fatigue during a marathon – you don’t say? Isn’t that generally a part of the experience?
I don’t have a good answer. I know I’ve had problems with this – I’m clearly in the high risk category for hyponatremia. I also generally have particularly poor races if it is a warm day.
My interventions include
1.) Drinking enough water
2.) Electrolyte supplements in my water (NUUN, Gu Brew)
3.) Additional electrolyte supplementation (SaltStick caps, Endurolytes caps, little pretzels)
4.) Making sure I have a salty snack or meal after a race or long run
5.) Trying to dress so I’m a little cool rather than a little warm
I’d love to read your suggestions – please leave a comment if you have any experience with hyponatremia and suggestions as to how to avoid it.
Most medical scientific organizations recommend low or moderate sodium diets to the general population in order to reduce the risk of high
blood pressure (hypertension).
Regular physical activity reduces the risk of hypertension.
Athletes lose sodium in sweat during exercise. The amount of sodium that is lost during endurance exercise depends on the sweating rate and
the concentration of sodium in the sweat. In turn, sodium loss during exercise depends on individual factors, such as genetics, fitness and heat
acclimatization, as well as the type, intensity and duration of exercise and the external environment.
Sodium ingestion by endurance athletes does not typically increase blood pressure, so low sodium diets are not recommended for individuals
who participate in long-term aerobic exercise.
Sodium ingestion during or following endurance exercise will help to stimulate thirst and drinking as well as stimulate fluid retention by the kidney.
No athletes are immune to hypertension, so athletes should monitor their blood pressure as they do their general health. This is particularly
important for older athletes, athletes with a genetic predisposition to hypertension, stroke or other cardiovascular disease.